Downloaded 132 times


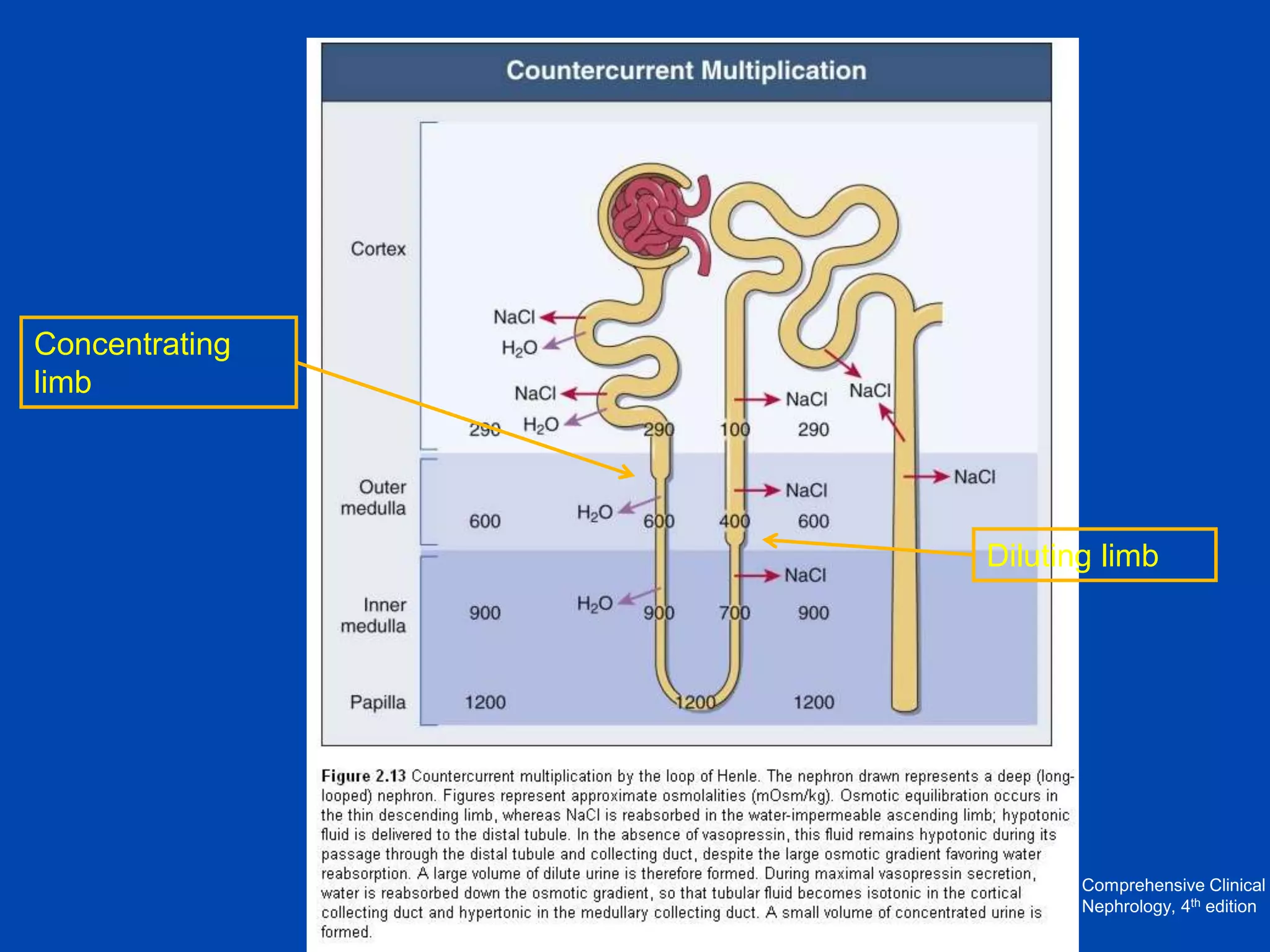
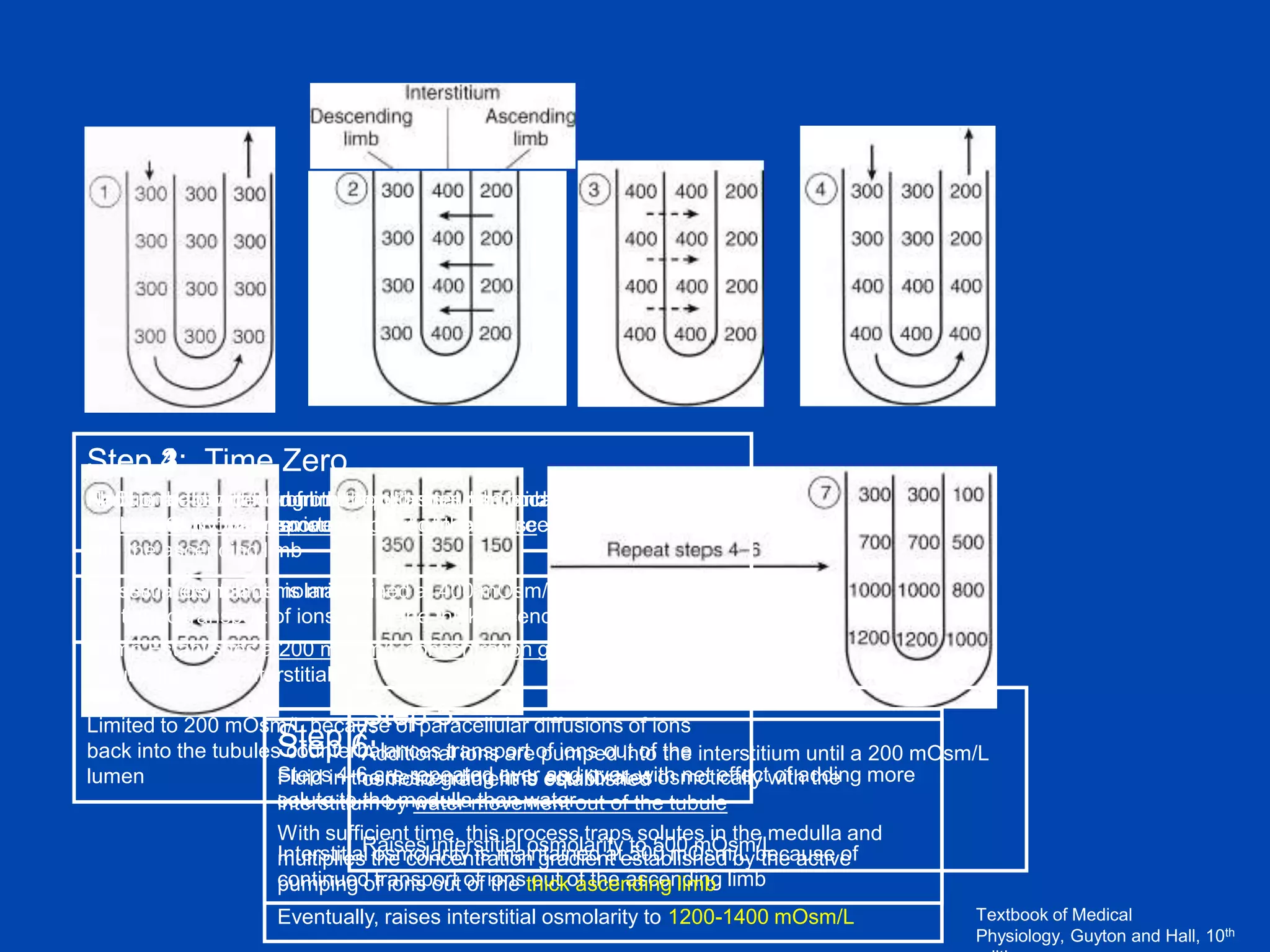

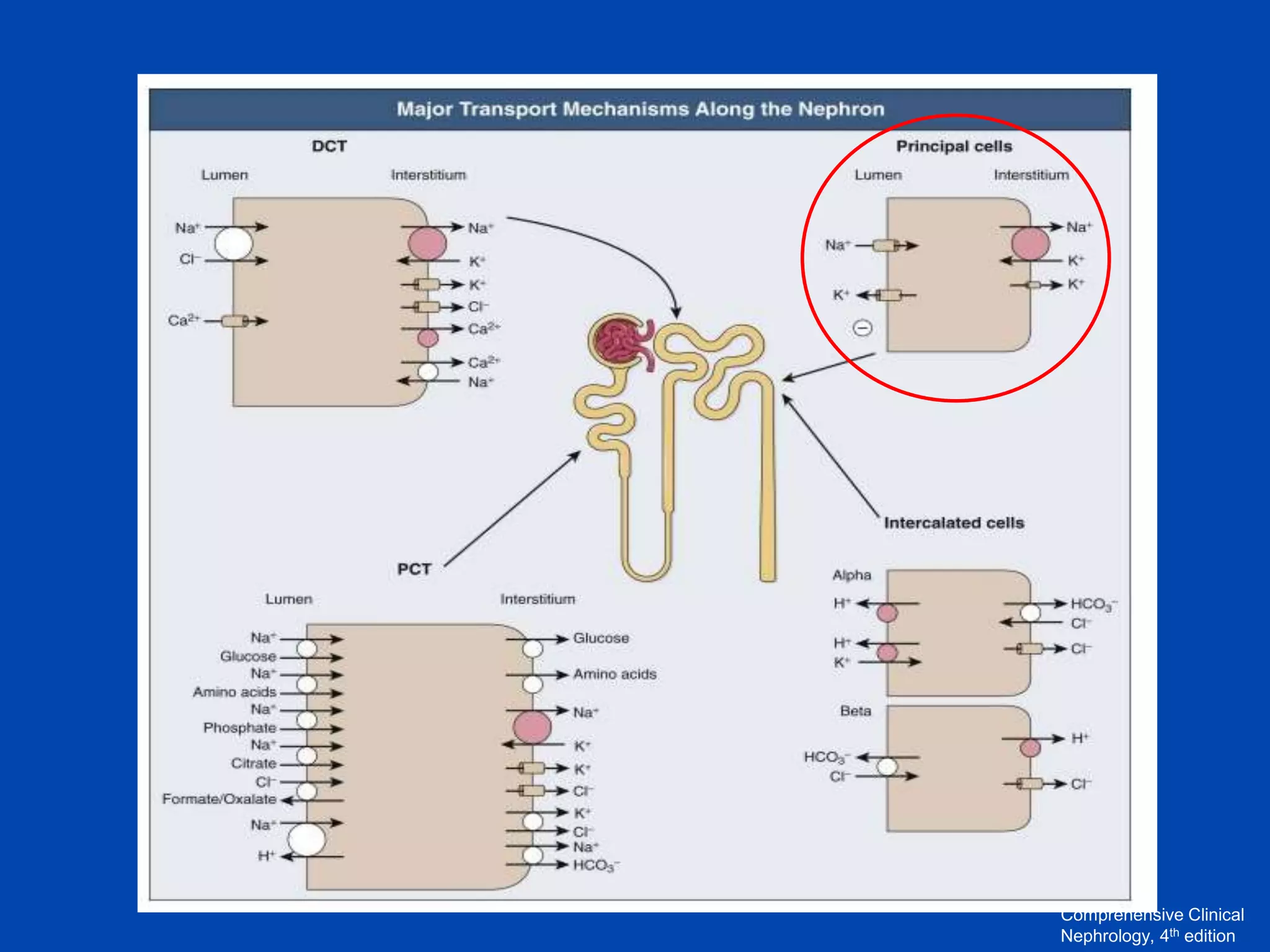
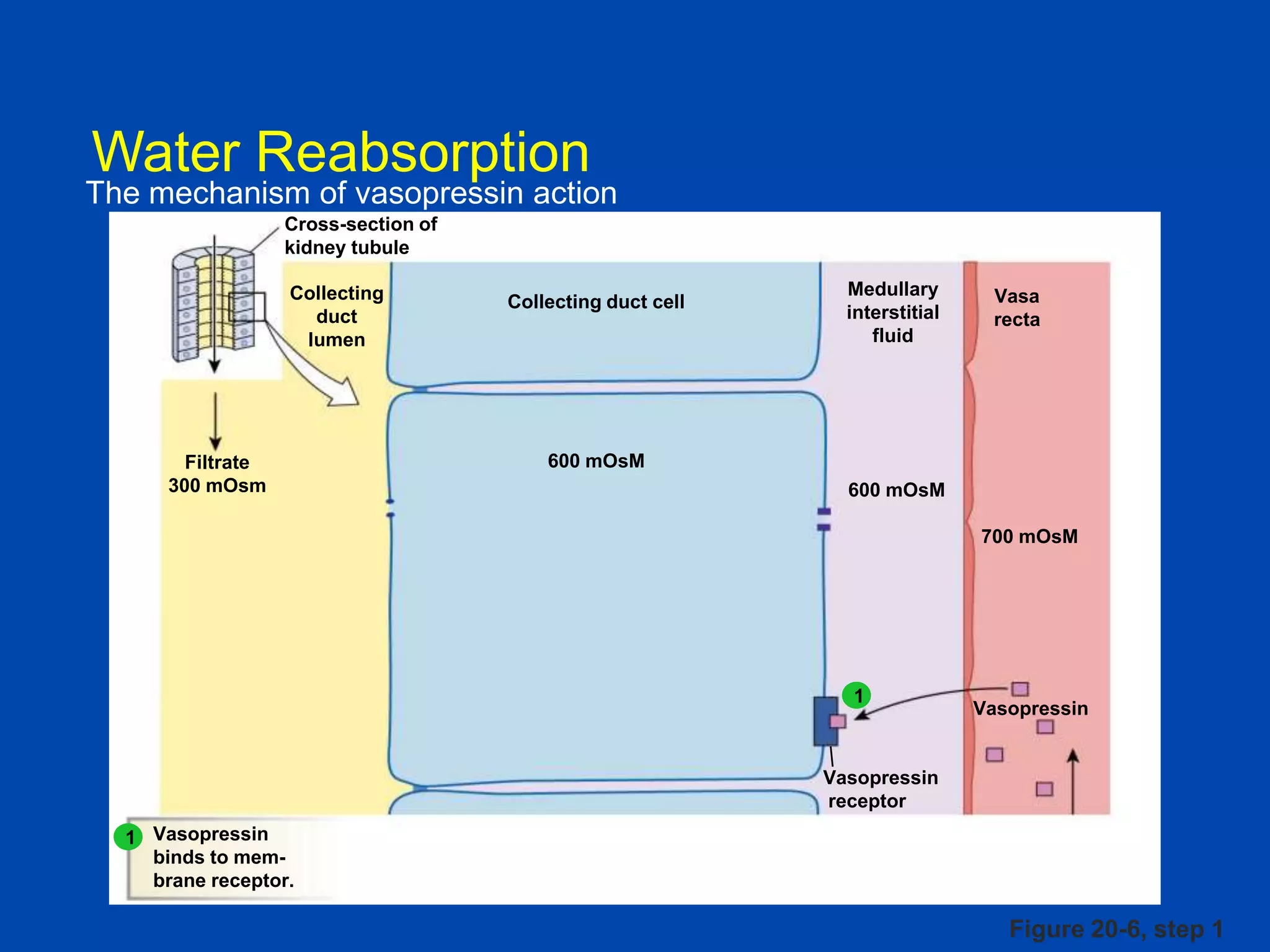
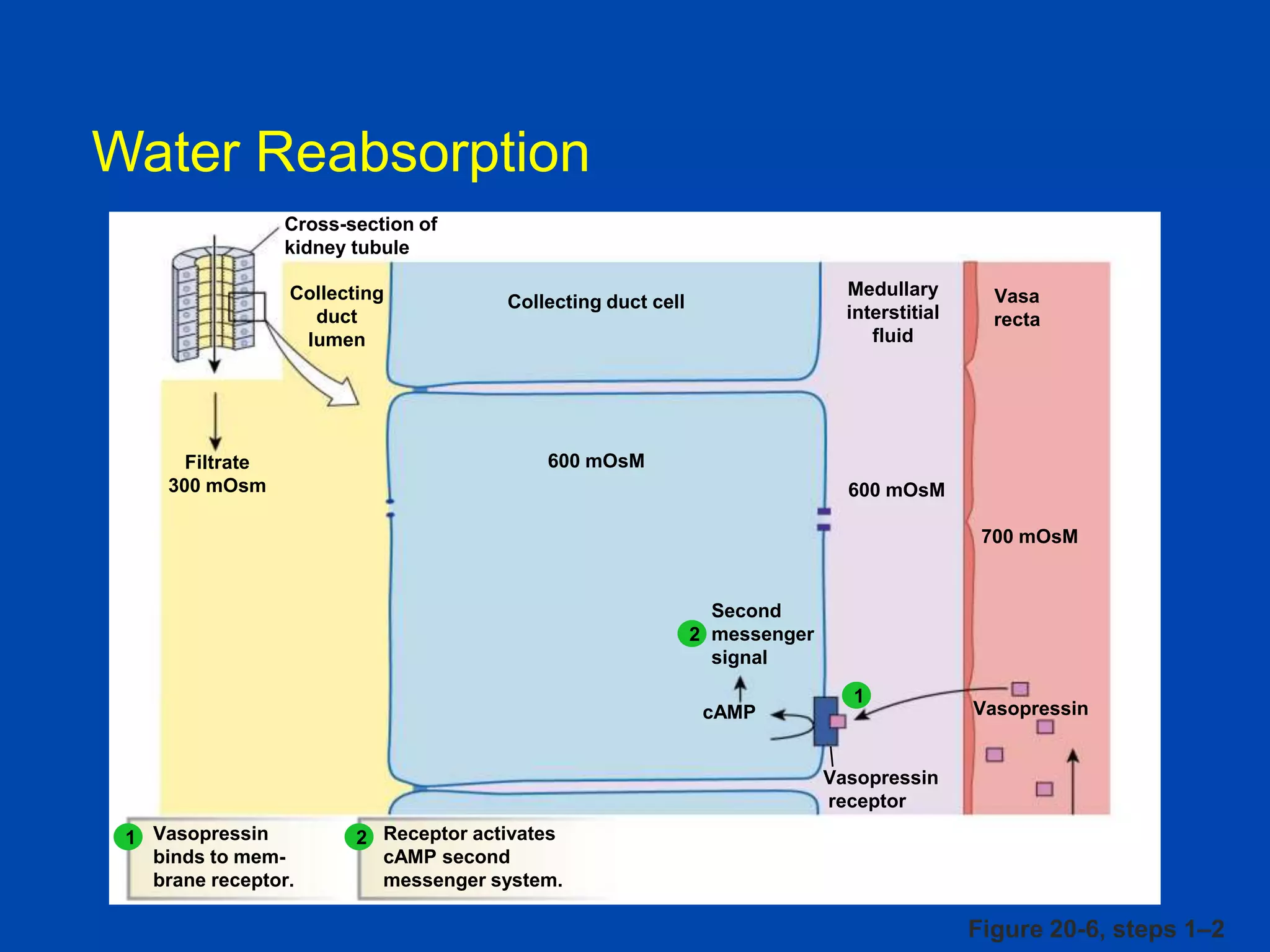
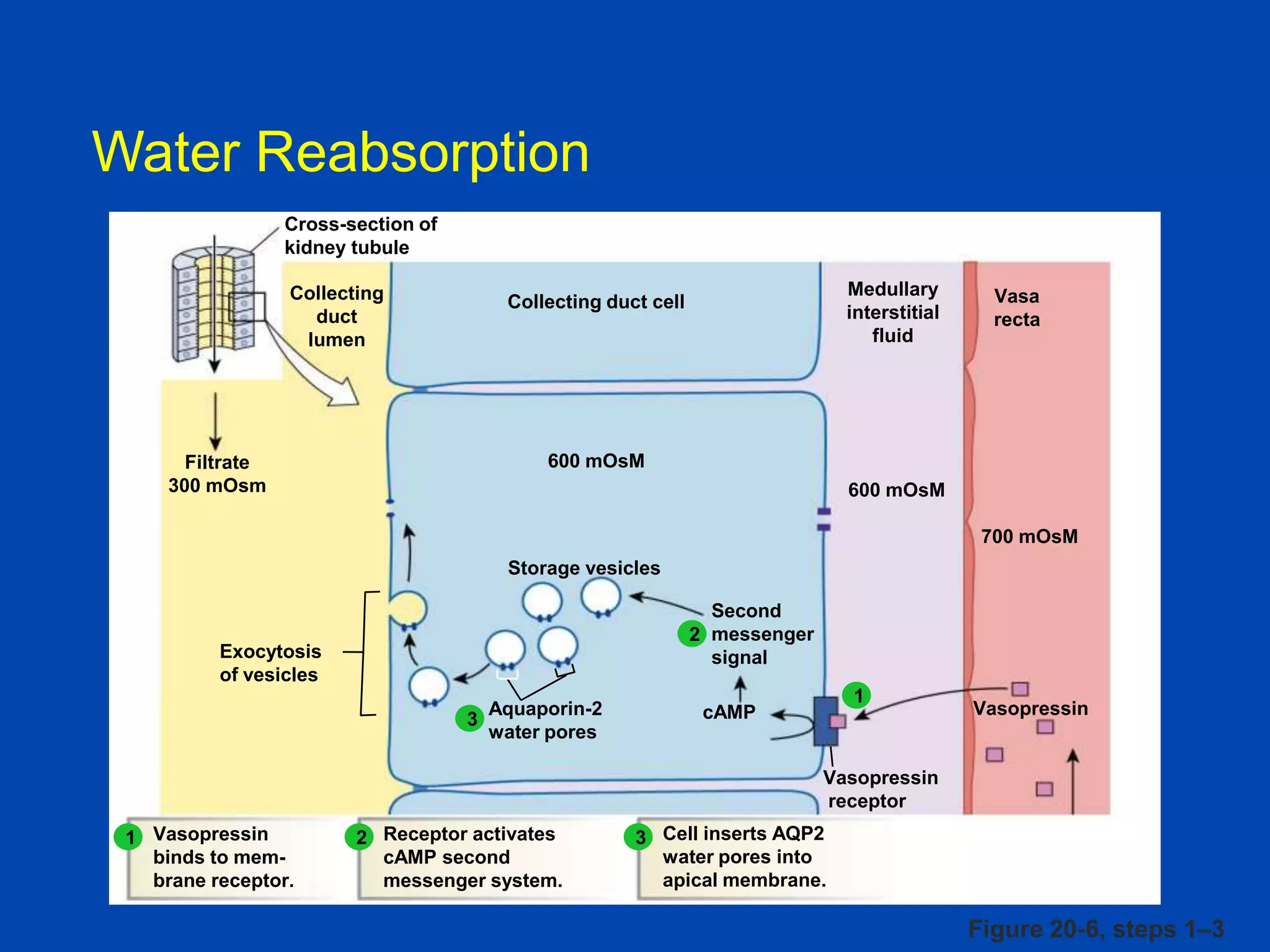
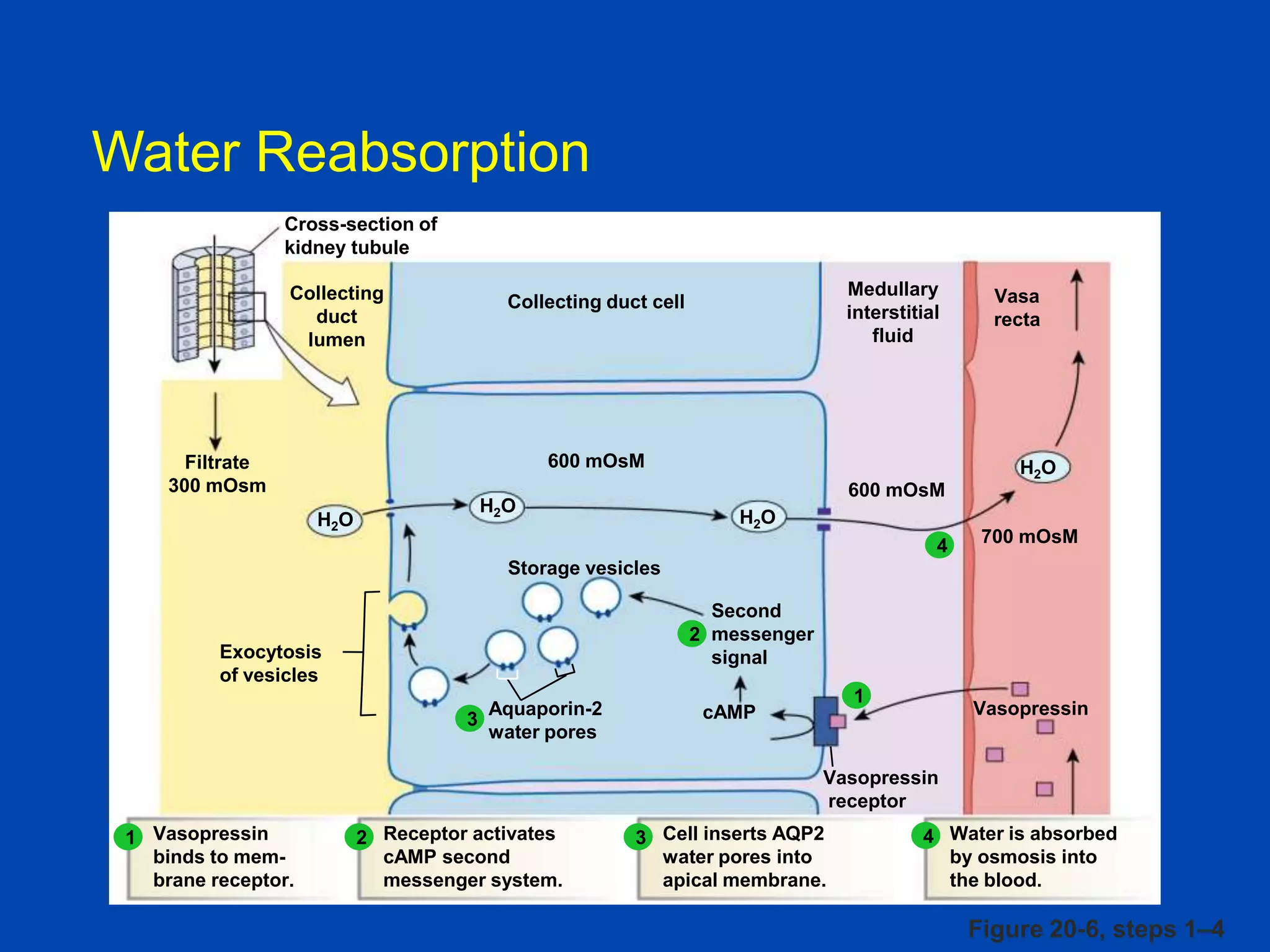
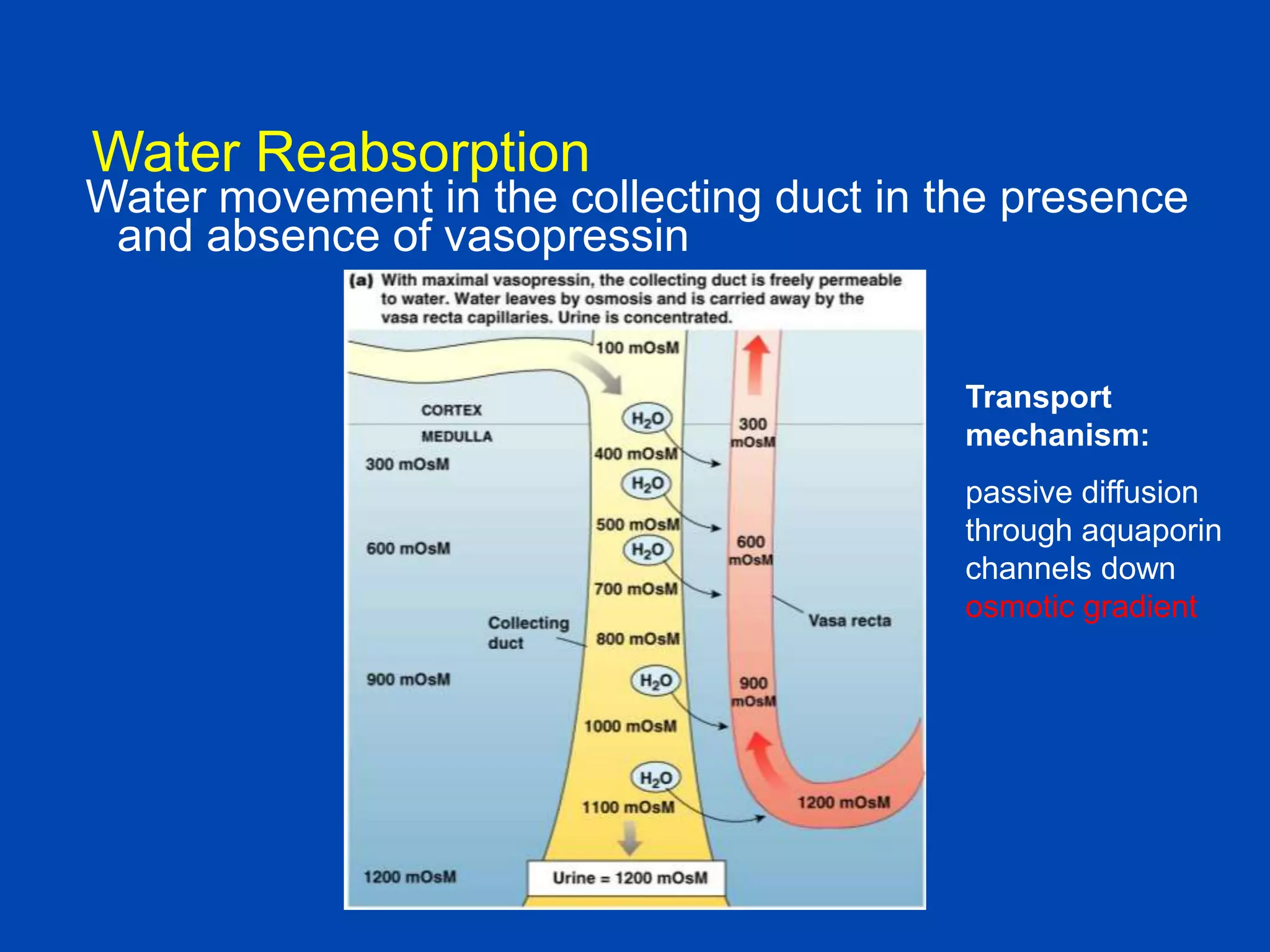

kidney tubule Collecting duct lumen Filtrate 300 mOsm Medullary interstitial fluid Collecting duct cell Vasa recta 600 mOsM 600 mOsM 700 mOsM 1. The kidney plays a pivotal role in maintaining water homeostasis by conserving water during deprivation and excreting excess water. This is accomplished through a complex anatomical arrangement of the nephron and renal vasculature. 2. Key elements include a hypertonic medullary interstitium generated by active transport of solutes out of the thick ascending limb of the loop of Henle and collecting


















































![Regulation of urine concentration and volume ].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/regulationofurineconcentrationandvolume-230418093129-e12f4cdf-thumbnail.jpg?width=640&height=640&fit=bounds)
























































