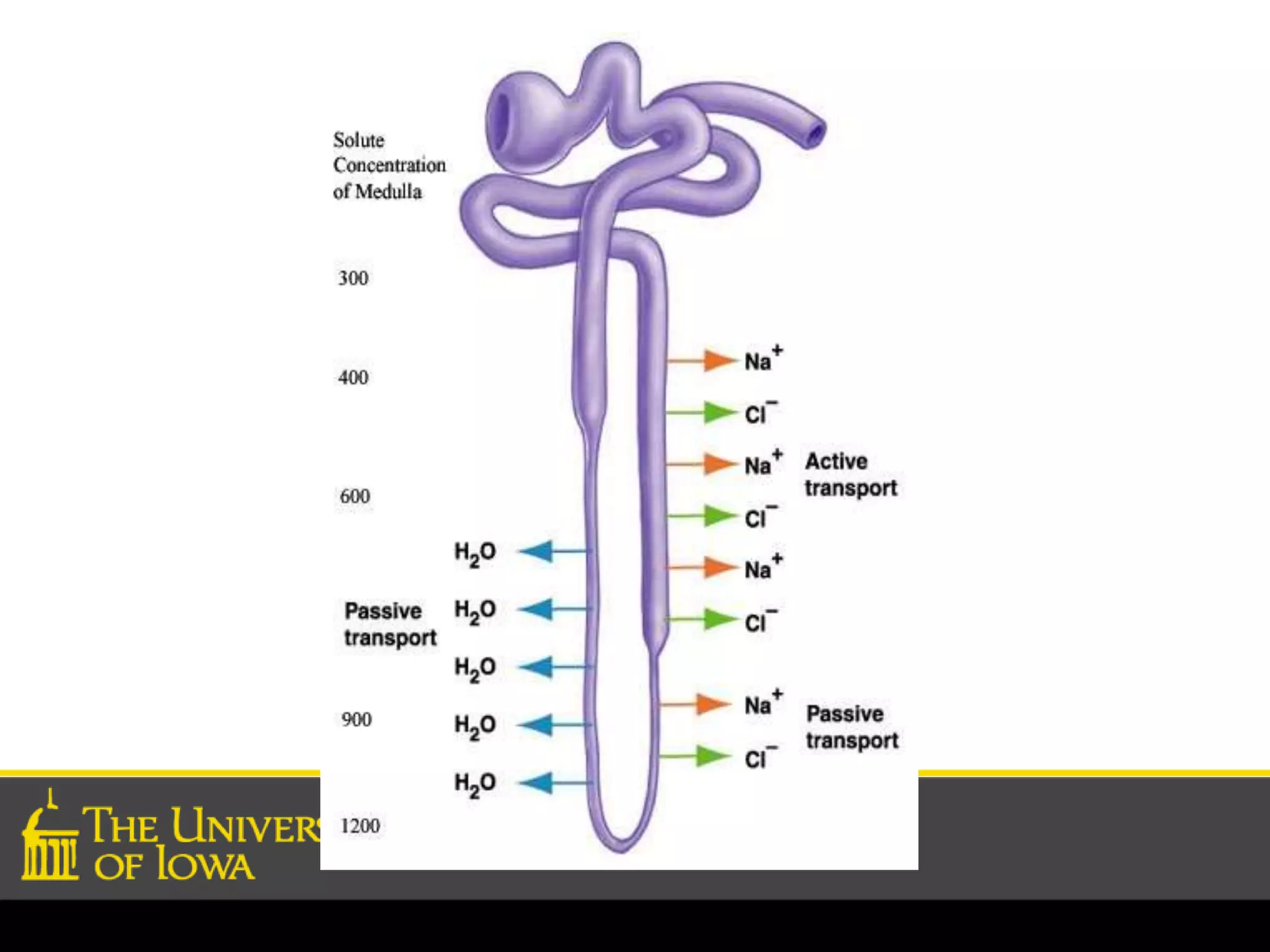

The document discusses the countercurrent multiplier mechanism in the kidney which allows it to concentrate urine. It describes how active transport of NaCl out of the thick ascending limb creates an osmotic gradient down the loop of Henle. As fluid moves through the thin descending limb, it becomes more concentrated due to water exiting into the hyperosmotic interstitium. The vasa recta help maintain this gradient by recycling urea and NaCl between the medulla and loop of Henle. Antidiuretic hormone regulates water reabsorption in collecting ducts to concentrate or dilute urine as needed. While the basic mechanism is understood, some aspects like solute transport in the thin descending limb and inner medulla remain unclear.
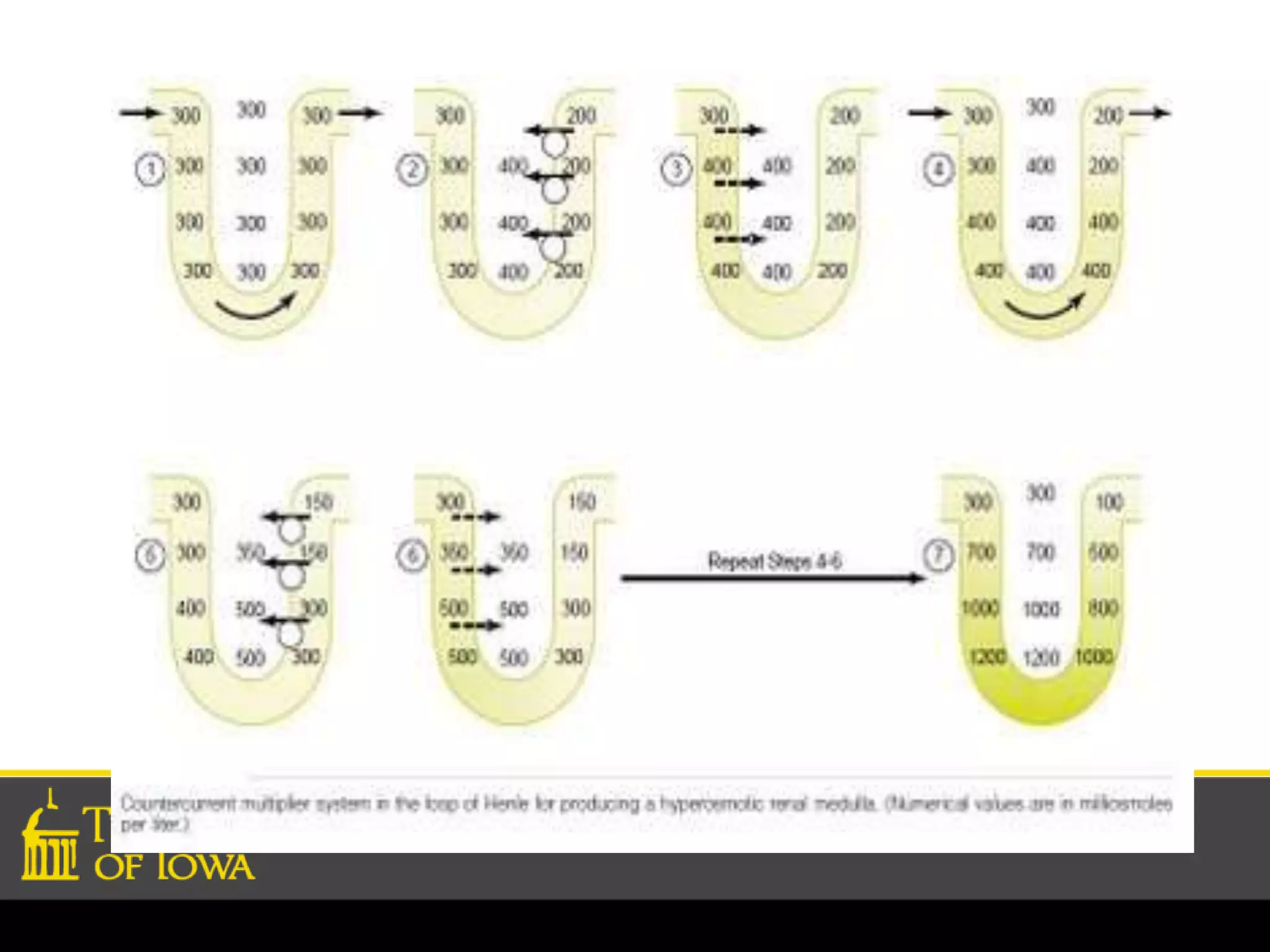
Introduction to the countercurrent multiplier mechanism in the kidney, often likened to a pyramid scheme.
Overview of kidney concentration mechanisms, highlighting roles of loops of Henle and current research.
Details on the concentrating ability, roles of loop of Henle, NaCl and urea's contributions.
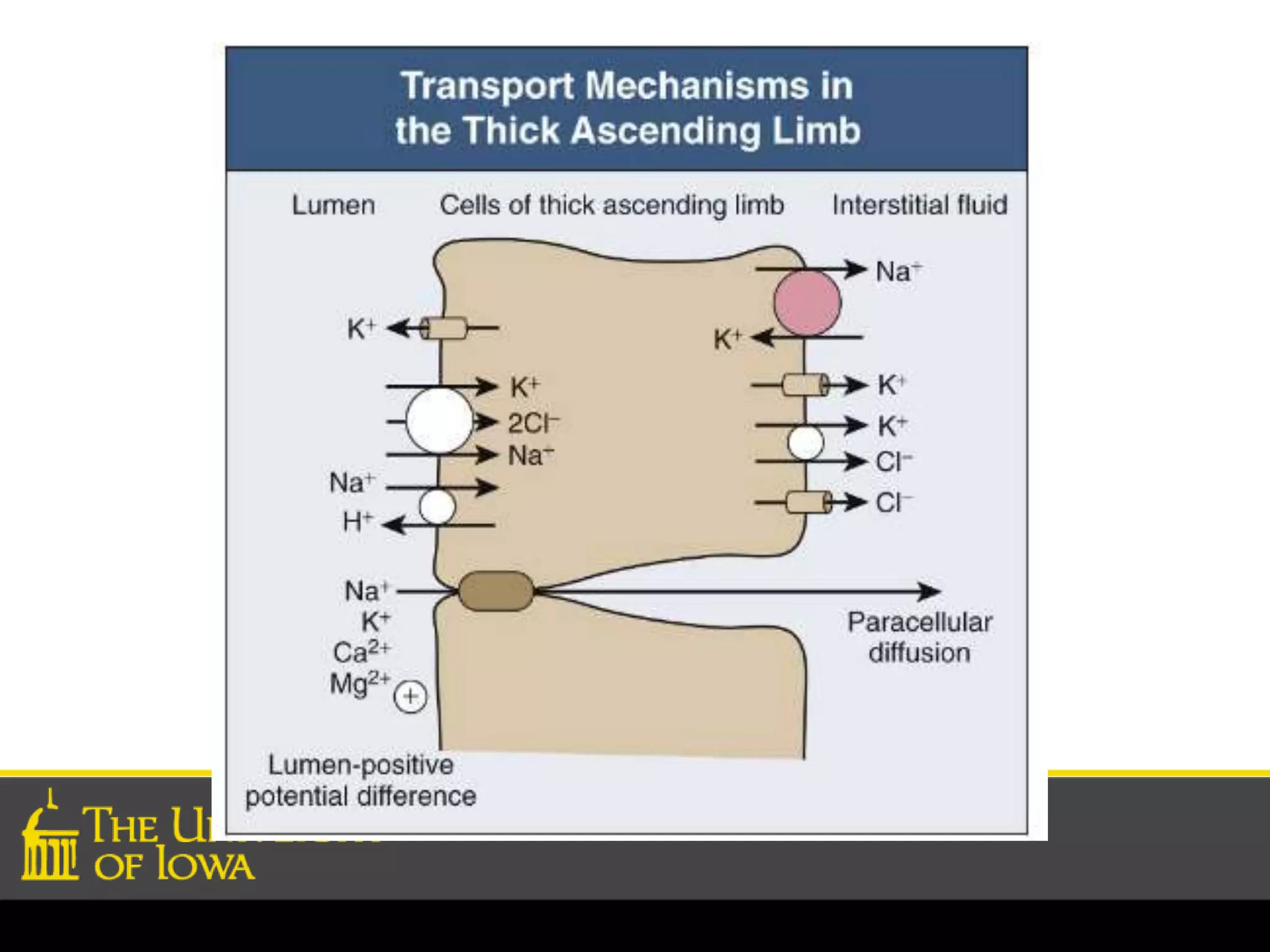
Function of the thick ascending limb in countercurrent multiplication and water reabsorption dynamics.
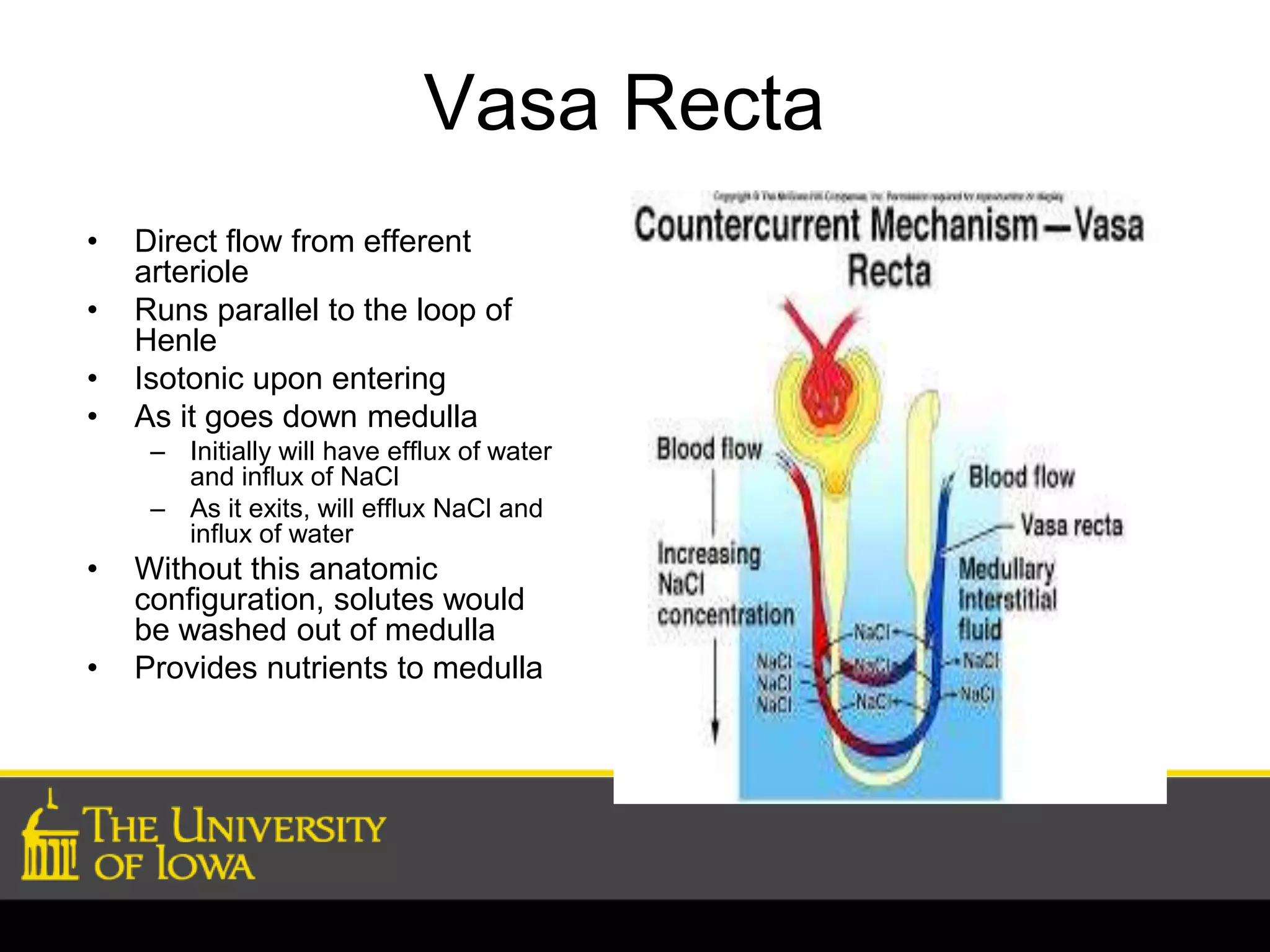
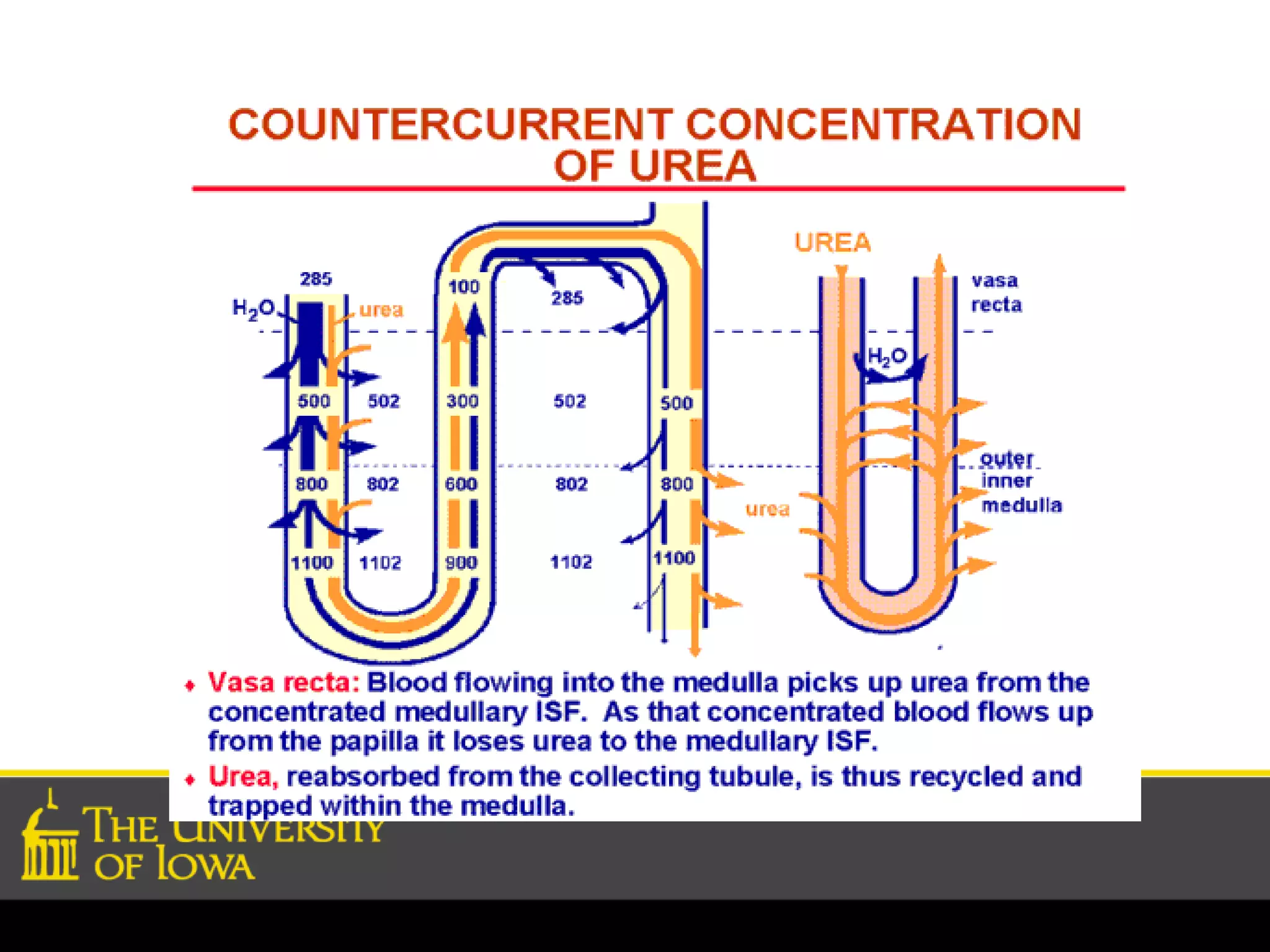
Vasa recta's anatomy and function in parallel to loops of Henle, maintaining medullary osmotic balance.
Role of urea in urine concentration, especially regarding its permeability in different kidney segments.
Mechanisms of antidiuresis involving ADH and subsequent water reabsorption in various kidney ducts.
Processes involved in diuresis leading to high volume, low concentration urine due to ADH absence.
Conditions impacting kidney's concentrating ability unrelated to ADH, causing sodium absorption issues.
Ongoing questions regarding solute handling in the kidney's inner medulla and transporters' roles.


































![Regulation of urine concentration and volume ].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/regulationofurineconcentrationandvolume-230418093129-e12f4cdf-thumbnail.jpg?width=640&height=640&fit=bounds)










![Renal Physiology. [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/renalphysiology-250924082023-9109186b-thumbnail.jpg?width=640&height=640&fit=bounds)








































