Downloaded 240 times
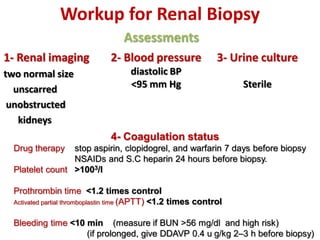
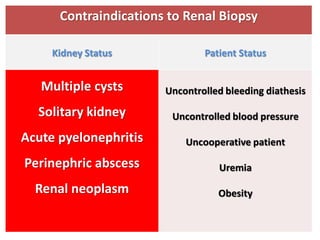
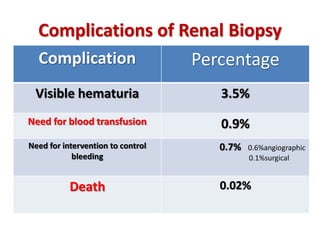



This document discusses renal biopsy procedures. It provides details on the history, technique, adequacy, contraindications, complications and indications for renal biopsy. Some key points include: - Renal biopsy has evolved since the 1950s and can now provide a tissue diagnosis in over 95% of patients with a life-threatening complication rate of less than 0.1%. - An adequate biopsy sample contains 10-15 glomeruli and provides samples for histology, immunofluorescence and electron microscopy. - Contraindications include bleeding diathesis and inability to comply with instructions. Relative contraindications include hypertension and infection. - Complications are rare but can include hematuria, pain, and rarely death from






















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











