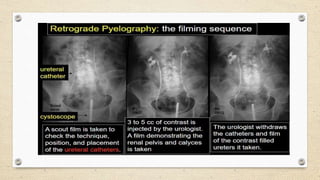
This document describes retrograde pyelography, a medical imaging procedure used to visualize the kidneys and ureters. It begins by introducing retrograde pyelography and its indications. These include evaluating the kidneys when normal visualization is not possible on other exams or when investigating hematuria, filling defects, or ureteral fistulas. The document then discusses patient preparation, anesthesia used, technique, required films, complications, and compares retrograde pyelography to other imaging modalities like MRI uretherography and CT urethrography. In summary, retrograde pyelography involves injecting contrast through ureters under fluoroscopy to visualize the pelvicalyceal system and evaluate various conditions of