Download as PDF, PPTX


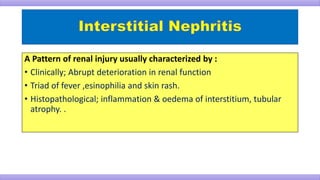
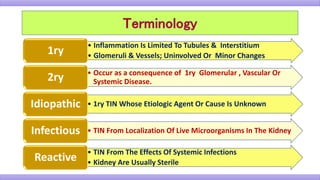
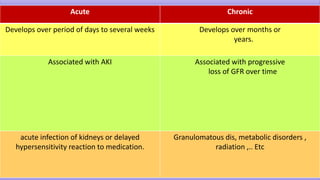
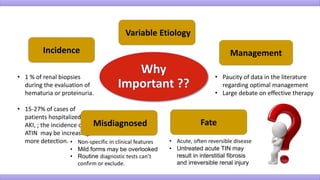
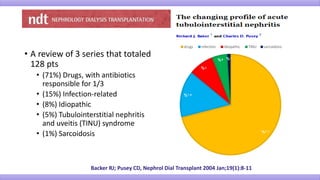


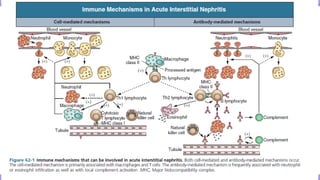
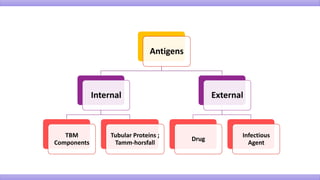

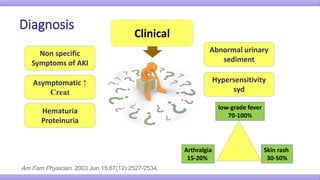

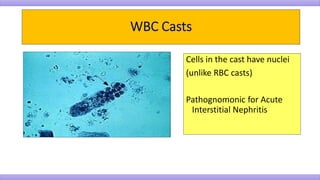
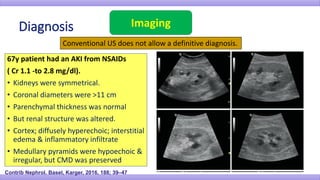


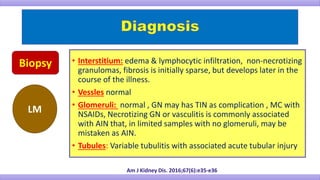
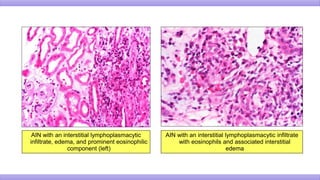
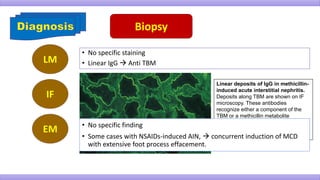


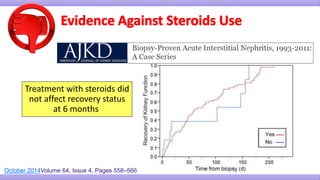
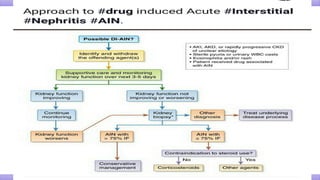
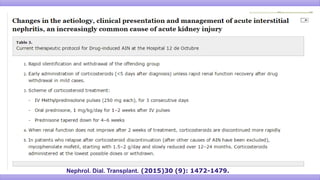
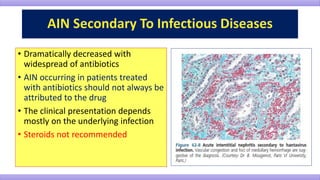
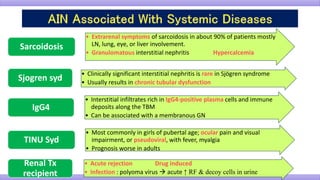


This document discusses tubulointerstitial nephritis (TIN), a pattern of renal injury characterized by inflammation and edema of the renal tubules and interstitium. TIN is most commonly caused by drugs (71% of cases) and infections (15% of cases). On biopsy, TIN shows lymphocytic infiltration of the tubules and interstitium with tubular atrophy and normal glomeruli and vessels. Treatment involves withdrawing the offending agent and supportive care. Corticosteroids may aid recovery but their effectiveness is debated. Prognosis depends on factors like duration of the insult and degree of fibrosis - complete recovery is more likely if treatment begins early.



















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



