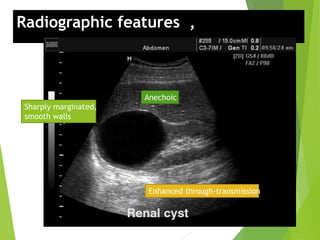
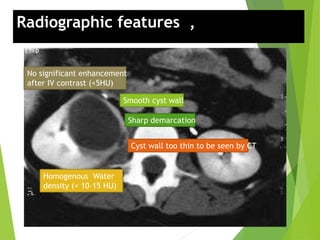
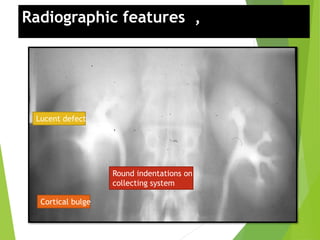
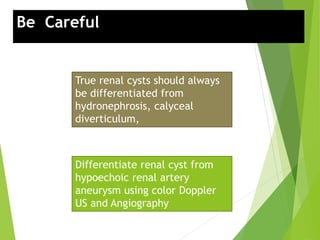
The document discusses simple renal cysts, which are fluid-filled sacs that are benign and commonly discovered incidentally in abdominal imaging. They may vary in number and size, and while usually asymptomatic, large cysts can cause discomfort or pain. The document also highlights investigation methods, differential diagnoses, and treatment options, emphasizing the importance of accurate diagnosis for appropriate management.