Downloaded 50 times
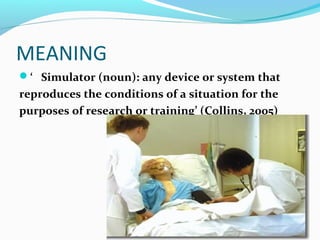
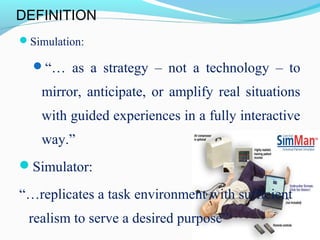

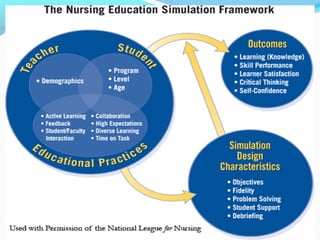
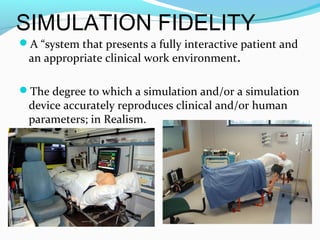

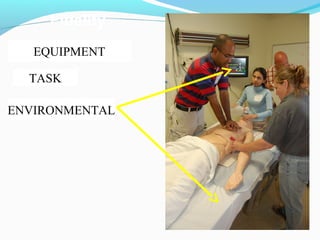
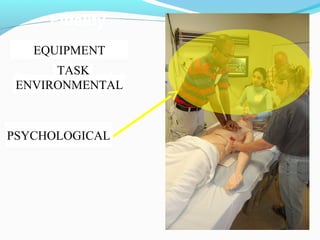
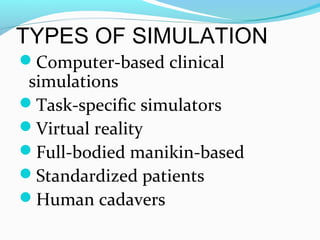
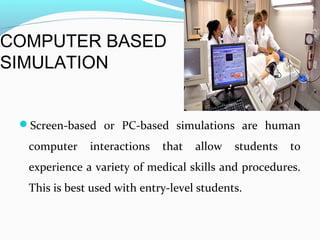
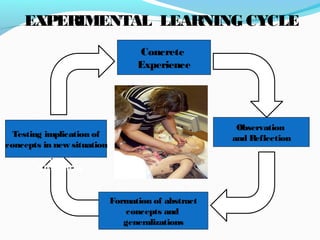



This document discusses simulation as a teaching strategy in nursing education. It defines simulation as replicating real situations to provide guided learning experiences. Simulation allows students to learn by doing in realistic environments. Debriefing after simulations is important for reflection and learning. The document outlines different types of simulations from computer-based to full-body mannequin to standardized patients. Higher fidelity simulations using mannequins provide more interactive and realistic learning experiences. Simulation aligns well with experiential learning theory and helps students apply concepts from concrete experiences.