Downloaded 47 times

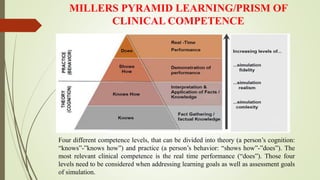
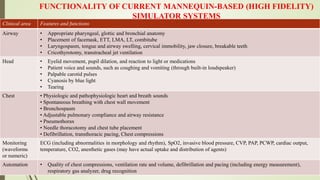

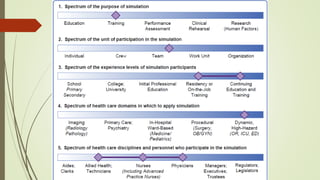
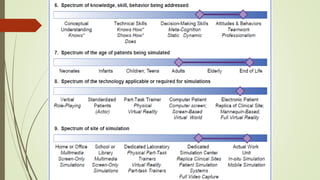


The document discusses simulation in medicine and its advantages. It describes Miller's pyramid of learning and the history of medical simulation. Simulation allows trainees to practice skills in a safe environment without risk to patients. It also allows rare scenarios to be replicated for learning. Current simulators range from part-task trainers to high-fidelity full-body mannequins that can replicate physical signs and physiological responses. The highest level of simulation incorporates simulated patients and environments to train technical and non-technical skills.