Downloaded 103 times







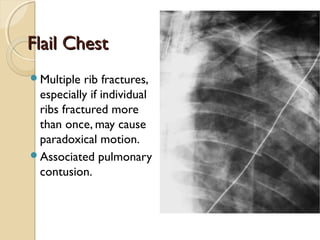

























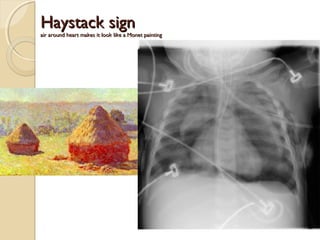






























This document discusses imaging of the chest in trauma patients. It describes the use of chest radiographs and CT scans to evaluate for fractures, dislocations, pneumothoraces, hemothoraces, pulmonary contusions and lacerations, diaphragm injuries, and vascular injuries following chest trauma. Key findings on imaging include rib fractures indicating underlying organ injury, flail chest, scapula fractures requiring CT, pneumothorax appearance varying with patient position, and indirect signs of aortic injury on CT such as mediastinal hematoma.









































![Chest_xray_in_trauma and trauma[PS].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/chestxrayintraumaps-250501045112-cc7e42ce-thumbnail.jpg?width=640&height=640&fit=bounds)



















































