Downloaded 39 times

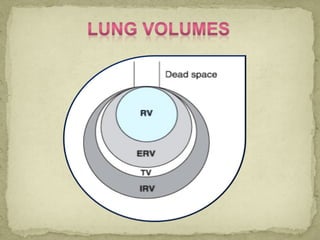
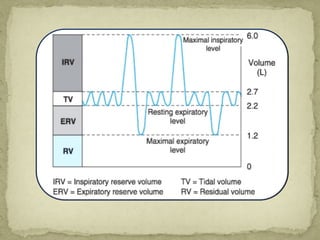
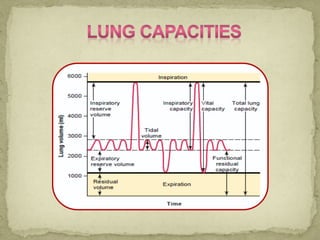



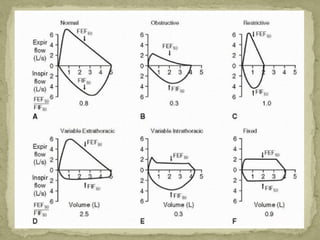
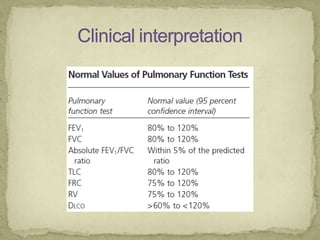
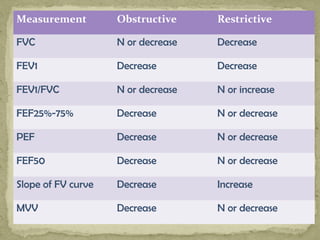
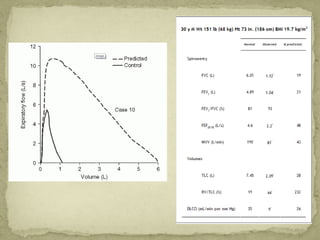

The document outlines pulmonary function testing (PFT), detailing its definition, purpose, indications, contraindications, and classifications of lung conditions. It explains how PFT evaluates lung function through various parameters, including lung volumes and capacities, and differentiates between obstructive and restrictive lung diseases. Additionally, it describes the interpretation of flow-volume curves and key respiratory metrics essential for clinical assessment.