Download as PDF, PPTX
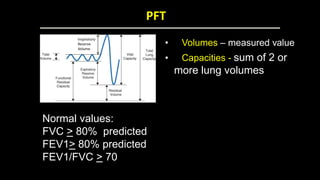
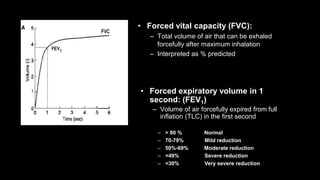
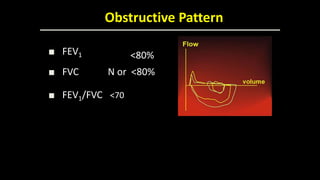
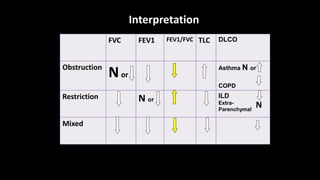
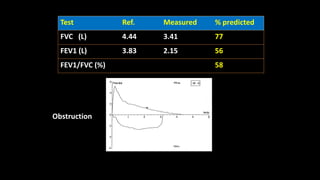
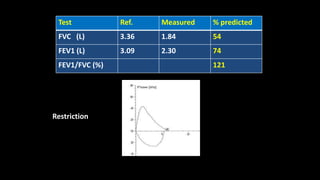
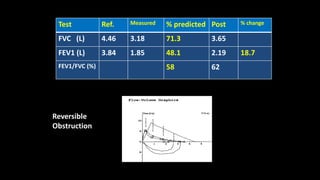
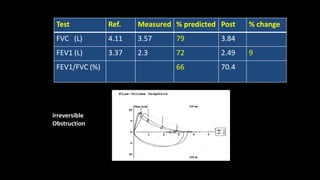
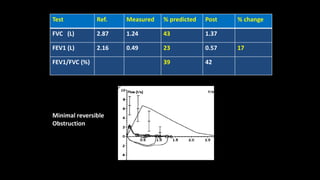
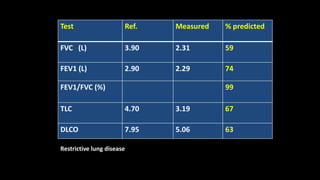

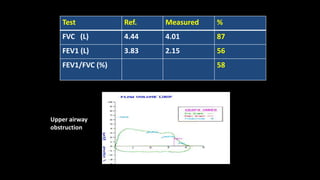
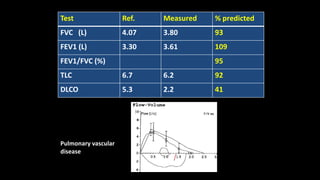
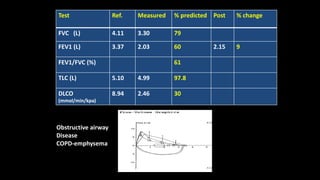
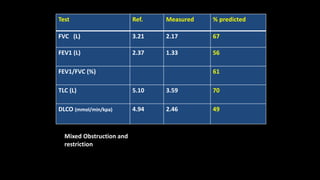
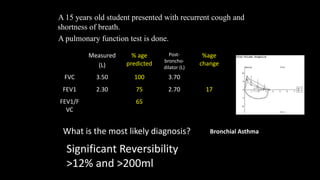
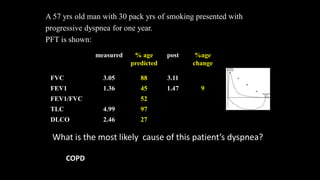


This document discusses pulmonary function tests (PFTs), including the types of tests performed and what each tests evaluates. It describes common PFT measurements like forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), their ratios, and how obstructive, restrictive, and mixed patterns are interpreted from PFT results. Examples of PFTs in different pulmonary diseases are provided along with interpretations.


































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


















