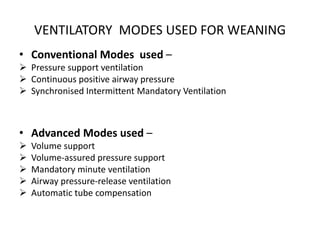
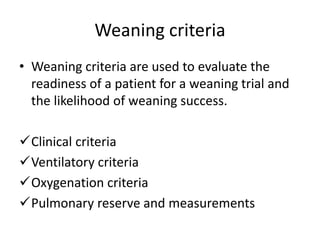
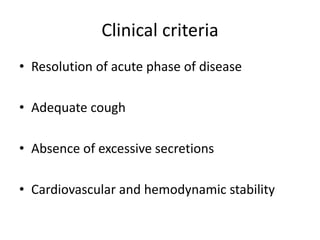
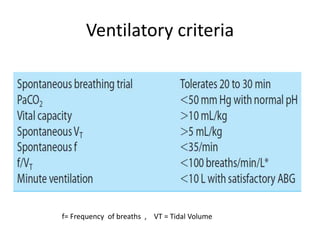
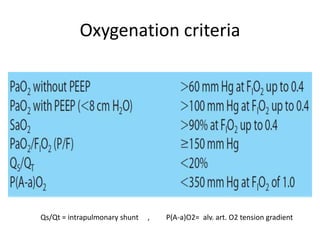
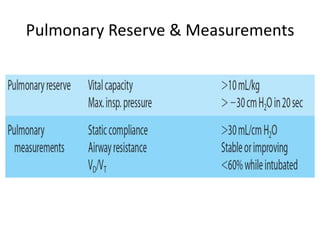
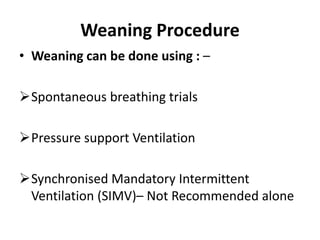
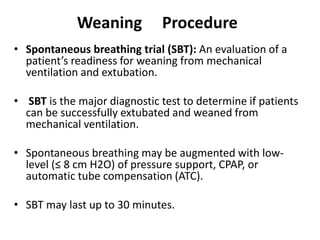
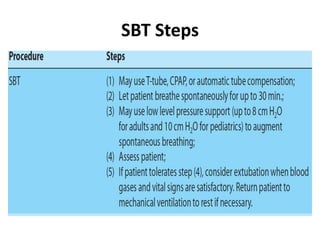
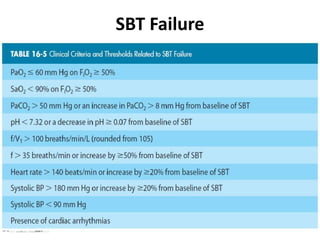
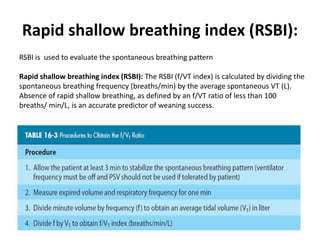
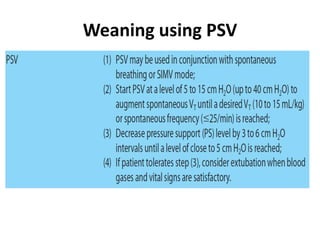
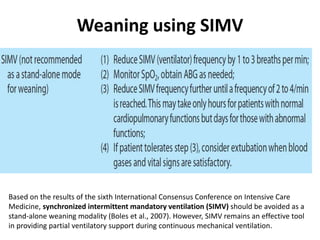
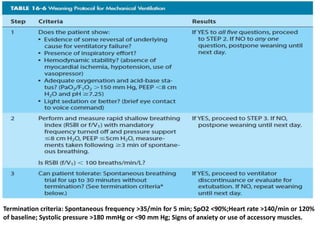
The document discusses weaning patients from mechanical ventilation. It begins by defining weaning as the process of withdrawing ventilator support and transferring breathing work to the patient. It states that patients must recover from their acute illness and be able to breathe spontaneously before weaning. Weaning is gradually started by evaluating clinical status and giving spontaneous breathing trials to assess readiness for extubation. Different ventilator modes used for weaning, like pressure support ventilation, are described. Weaning criteria involving clinical, ventilatory, oxygenation, and pulmonary measurements are provided to determine weaning success. The weaning procedure, including spontaneous breathing trials and parameters like the rapid shallow breathing index to predict weaning outcome, are outlined. Causes of we







































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















