Downloaded 18 times

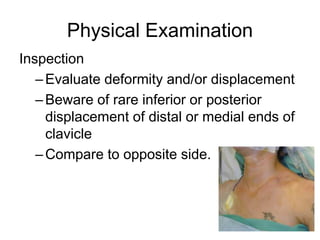
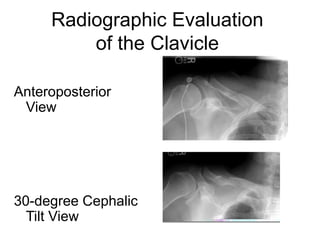

Clavicle fractures most commonly occur in the middle third of the clavicle and result from a direct impact to the shoulder. Physical examination involves inspecting for deformity and comparing to the opposite clavicle, as well as evaluating pain and instability. Radiographic imaging, including anteroposterior and 30-degree cephalic tilt views, is used to classify fractures by their location and degree of displacement. Treatment options include nonoperative management with slings and braces or surgical fixation using plates, screws, pins, or titanium elastic nails. Following treatment, physiotherapy focuses on education, rest, bracing, electrotherapy, taping, and graduated exercises to improve posture, flexibility, strength, and return to