
Download to read offline





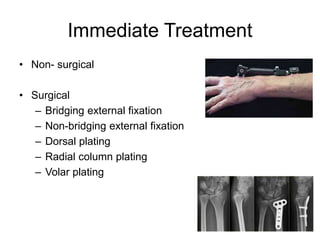


Distal radius fractures are among the most common upper extremity fractures. They represent about one-sixth of all emergency department fractures. Risk factors in the elderly include low bone density, female sex, and falls from standing height. Clinically, there is wrist deformity, swelling, and pain with motion. Radiographs of the wrist and potentially the elbow are needed to classify and further evaluate the fracture. Treatment may involve casting, external fixation, or plating depending on the fracture type and location. Rehabilitation aims to control symptoms and regain range of motion and strength.























































































