Downloaded 11 times





























![CLINICAL USE OF FLOW-VOLUME LOOP
• detection of obstruction of the upper airway
Three distinct patterns:
• variable extrathoracic obstruction,
• variable intrathoracic obstruction, and
• fixed obstruction
• the contour of the flow-volume loop can provide additional
information about the location of airway constriction,
• the sensitivity is low for mild obstruction and interpretation
can be hampered by overlapping diseases (eg, chronic
obstructive pulmonary disease [COPD] and tracheal stenosis).
• Thus, positive and negative findings should be confirmed with
imaging and/or direct visualization. 2021 UPTODATE®](https://image.slidesharecdn.com/spirometry-220604142109-14c5c592/75/Spirometry-37-2048.jpg)












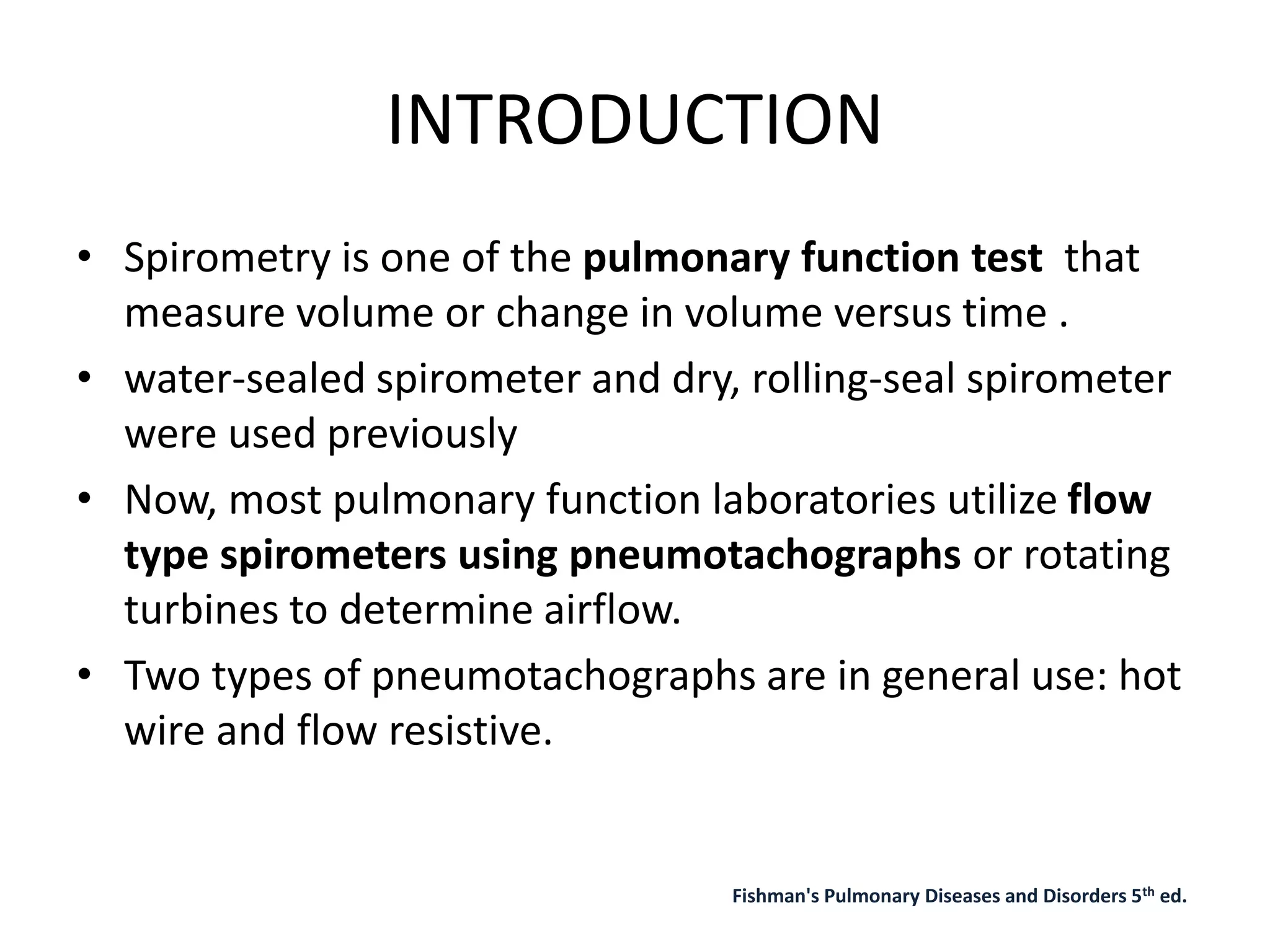
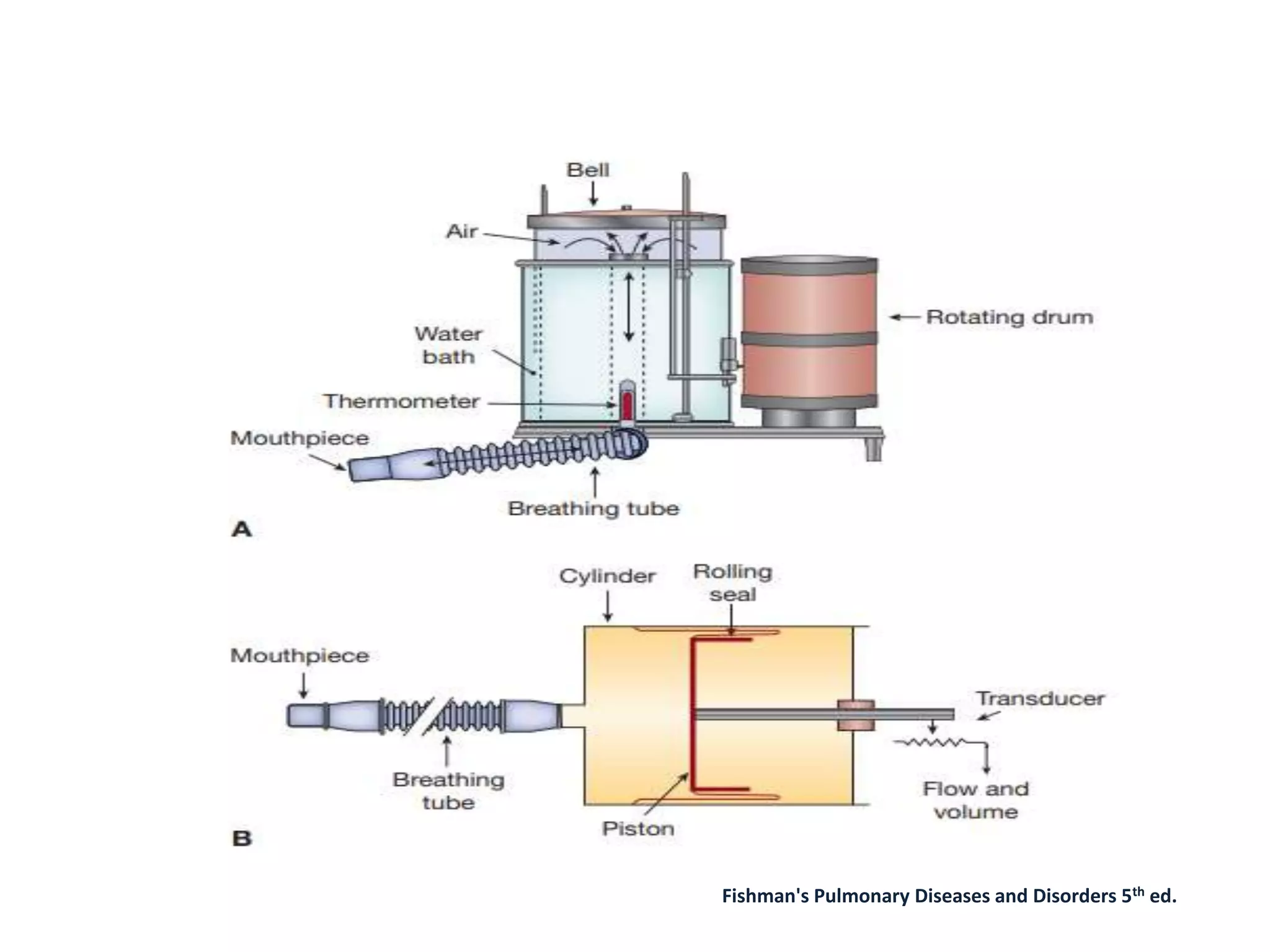
Spirometry measures lung volumes and airflow. Modern spirometers use flow sensors to measure tidal volume, inspiratory reserve volume, expiratory reserve volume, residual volume, vital capacity, and total lung capacity. Key metrics include FEV1, FVC, and their ratio. Spirometry is used to diagnose and monitor lung diseases, assess surgical risk, and evaluate therapeutic interventions. Proper technique requires full inspiration and expiration over 6 seconds. Results are interpreted by comparing values to predicted norms and assessing for reversibility of obstruction.
















































































