Downloaded 52 times

![References
• Doll R, Peto R: The causes of cancer: quantitative estimates of avoidable risks of cancerin the United States
today.
• JNatlCancer Inst 1981, 66:1191-1308. PubMed Abstract
• Harvard Report on CancerPrevention. Volume 1: Causes of human cancer
• Cancer Causes Co ntro l 1996, 7(Suppl 1):S3-59. PubMed Abstract | Publisher Full Text
• World Cancer Research Fund/American Institutefor Cancer Research: Fo o d, nutritio n and the preventio n o f cancer: A
glo bal perspective. Washington, DC: American Institutefor Cancer Research; 1997.
• Colditz GA, Atwood KA, EmmonsK, Monson RR, Willett WC, TrichopoulosD, Hunter DJ:Harvard report on cancer
prevention volume 4: Harvard cancerrisk index.
• Cancer Causes Co ntro l 2000, 11:477-488. PubMed Abstract | Publisher Full Text
• World Health Organization: WHO technical reports series 916. Diet, Nutrition, the prevention of chronic
disease. In Repo rt o f a jo int WHO/FAO Expert Co nsultatio n. Geneva: WHO; 2003.
• BoyleP, Autier P, Bartelink H, BaselgaJ, BoffettaP, Burn J, BurnsHJ, Christensen L, DenisL, Dicato M, Diehl V, Doll
R, Franceschi S, GillisCR, Gray N, GriciuteL, Hackshaw A, Kasler M, KogevinasM, Kvinnsland S, LaVecchiaC, Levi
F, McVieJG, MaisonneuveP, Martin-Moreno JM, Bishop JN, Oleari F, Perrin P, Quinn M, RichardsM, Ringborg U,
Scully C, SirackaE, Storm H, TubianaM, Tursz T, Veronesi U, Wald N, Weber W, ZaridzeDG, Zatonski W, zur Hausen
H: European Code Against Cancerand scientific justification: (third version 2003).
• Ann Onco l 2003, 14:973-1005. PubMed Abstract | Publisher Full Text
• National Cancer Center Tokyo Japan: Twelve recommendations forcancerprevention. [
http://www.ncc.go.jp/jp/ncc-cis/pub/index/about.html] webcite
• Japan Health Promotion and FitnessFoundation Tokyo Japan: Healthy People Japan 21.[
http://www.kenkounippon21.gr.jp/] webcite
• WardleJ, Waller J, Brunswick N, JarvisMJ: Awareness of risk factors forcanceramong British adults.
• Public Health 2001, 115:173-174. PubMed Abstract | Publisher Full Text
• Breslow RA, Sorkin JD, Frey CM, Kessler LG: American's knowledge of cancerrisk and survival.
• Prev Med 1997, 26:170-177. PubMed Abstract | Publisher Full Text
• PohlsUG, Renner SP, Fasching PA, Lux MP, KreisH, Ackermann S, Bender HG, Beckmann MW: Awareness of
breast cancerincidence and risk factors among healthy women.
• Eur JCancer Prev 2004, 13:249-256. PubMed Abstract | Publisher Full Text
• Keighley MR, O'Morain C, GiacosaA, Ashorn M, BurroughsA, Crespi M, Delvaux M, FaivreJ, Hagenmuller F, Lamy
V, Manger F, MillsHT, Neumann C, Nowak A, Pehrsson A, SmitsS, Spencer K, United European Gastroenterology
Federation Public AffairsCommittee: Public awareness of risk factors and screening forcolorectal cancerin
Europe.](https://image.slidesharecdn.com/publicawarenesstarekaminlecturei-140501101048-phpapp02/85/Public-awareness-41-320.jpg)

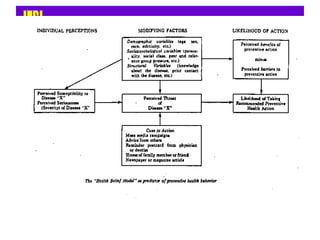
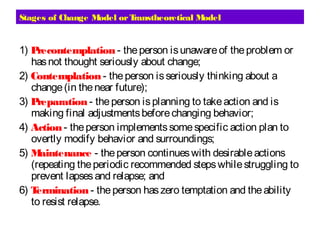
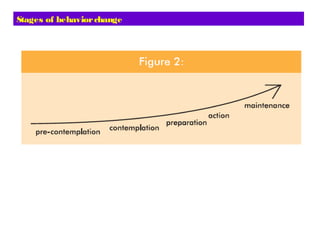
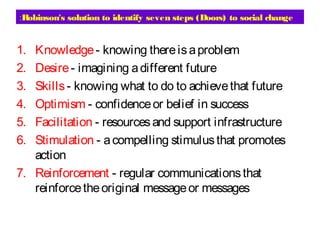
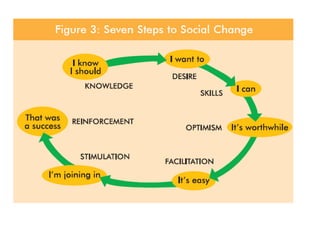
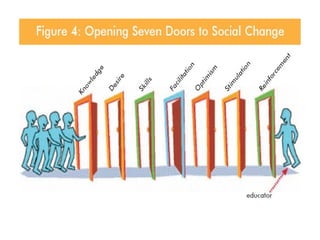
This document discusses concepts related to public awareness and health education. It begins by outlining objectives of recognizing the concept of public awareness, basic components of communication and education processes, and health education theories. It then provides details on raising public awareness, including that the process must meet mutual needs and influence community attitudes/behaviors. Key approaches to awareness raising are discussed, including personal communication, mass communication, education, and advocacy. Several behavioral models are examined at the individual, interpersonal, and community levels, including the health belief model, stages of change model, diffusion of innovations theory, and community organization approach. Communication challenges and factors influencing complexity are also reviewed.














































































![Medical statistics Basic concept and applications [Square one]](https://cdn.slidesharecdn.com/ss_thumbnails/medicalstatisticsl123m-131208222631-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)











![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











