Downloaded 294 times


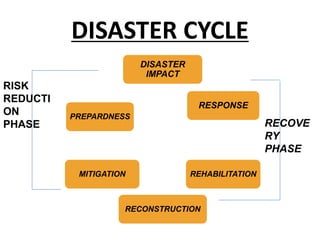



















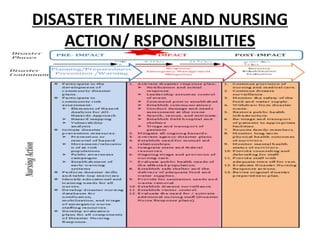











This document discusses disaster management and is divided into several sections. It defines disasters and hazards, and classifies disasters into 5 categories including water/climate, geological, chemical/industrial, accident, and biological disasters. It describes the disaster cycle and impact/response phase, which involves search and rescue, triage, tagging victims, and caring for the dead. The relief phase focuses on disease control, nutrition, vaccination, and rehabilitation. Other sections cover the recovery, preparedness, and planning phases of disaster management.

















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




