Downloaded 48 times

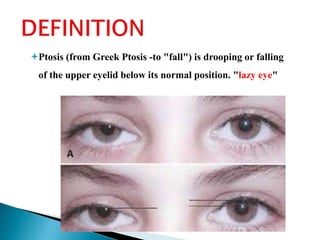
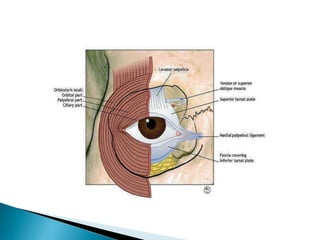
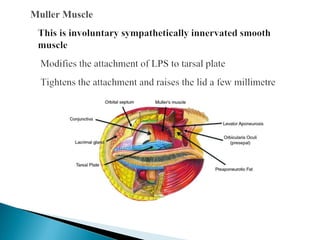
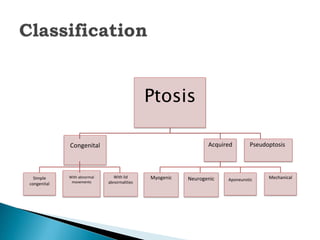
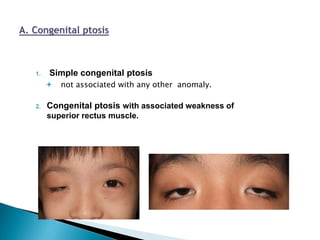
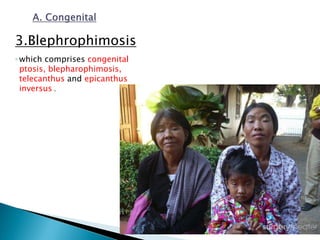

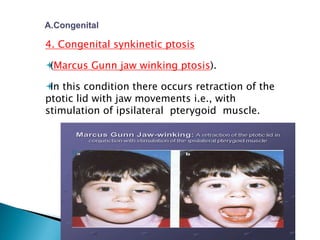
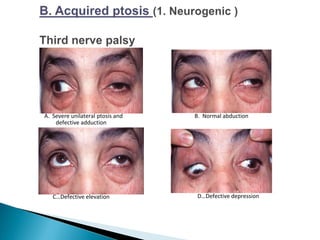
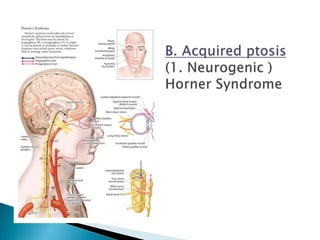
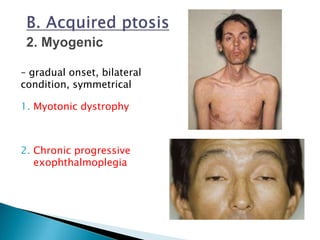
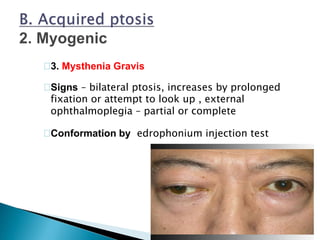
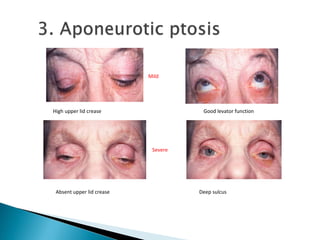
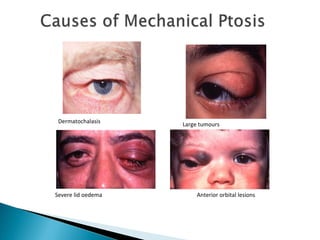
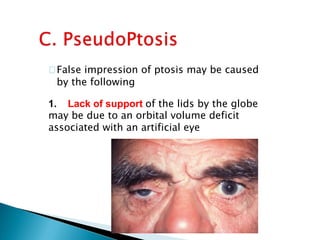
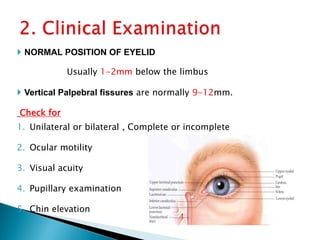


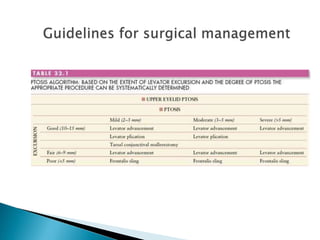
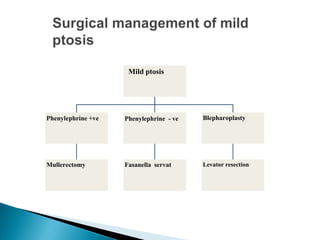
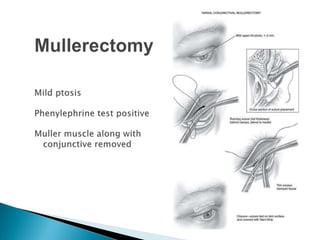

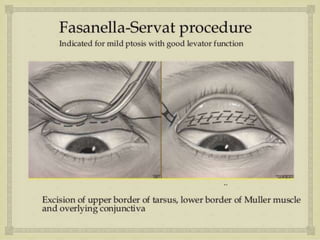

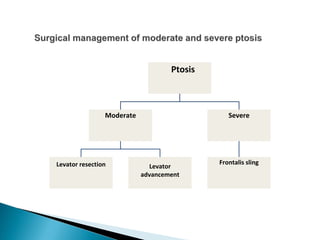
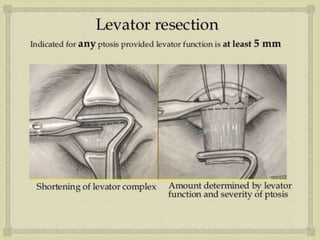

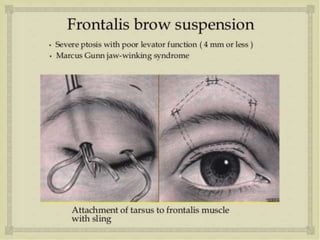
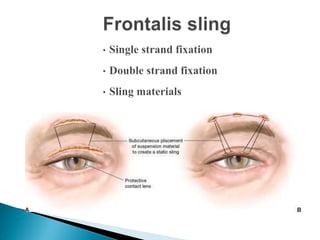






The document discusses ptosis, a condition characterized by the drooping of the upper eyelid, detailing its definition, classifications, clinical features, diagnostic methods, and treatment options. It includes congenital types, neurogenic and myogenic forms, and management strategies ranging from non-surgical interventions to various surgical techniques. Diagnosis relies on a thorough assessment of eyelid position, muscle function, and associated ocular anomalies.



































![CLINICAL EVALUATION AND MANAGEMENT OPTION OF AQUIRED PTOSIS [Autosaved]_09133...](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalevaluationandmanagementoptionofaquiredptosisautosaved091336-250701164538-7d28272b-thumbnail.jpg?width=640&height=640&fit=bounds)

























![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





