Downloaded 16 times

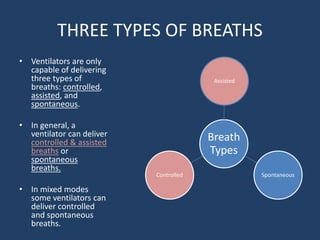




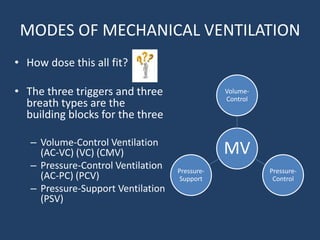
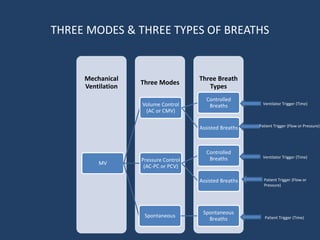
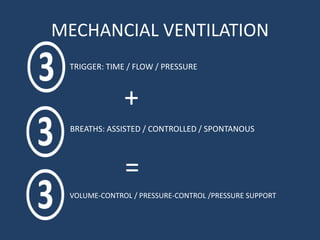


The document explains mechanical ventilation, outlining three triggers (time, flow, pressure) that initiate the respiratory cycle, and the three types of breaths (controlled, assisted, spontaneous) that ventilators can deliver. It describes how these concepts integrate into three ventilation modes: volume-control, pressure-control, and pressure-support. The content serves as foundational knowledge for understanding mechanical ventilation systems and their clinical applications.


![Dual controlled modes of mechanical ventilation [onarılmış]](https://cdn.slidesharecdn.com/ss_thumbnails/dualcontrolledmodesofmechanicalventilationonarlm-151116121024-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)










































































