Download as PDF, PPTX


















































































This document provides an overview of lung cancer, including: - The four most common causes of lung masses are benign lesions, primary lung cancer, metastatic disease, and lung abscess. - There are two main types of lung cancer - small cell lung cancer and non-small cell lung cancer, which is most common. - Symptoms of lung cancer can include cough, breathing problems, weight loss, chest pain, and fatigue, though early-stage cancers may be asymptomatic. - Diagnostic tests include chest x-rays, CT scans, sputum cytology, bronchoscopy, and biopsies. Staging helps determine prognosis and treatment.
An overview of practical approach to lung cancer by Dr. Gamal Rabie Agmy. Relevant credentials.
Focus on lung masses, including causes like benign lesions, primary lung cancer, metastatic disease, and lung abscess.
Characteristics of benign lung masses: small size, calcified density, well-defined margins.
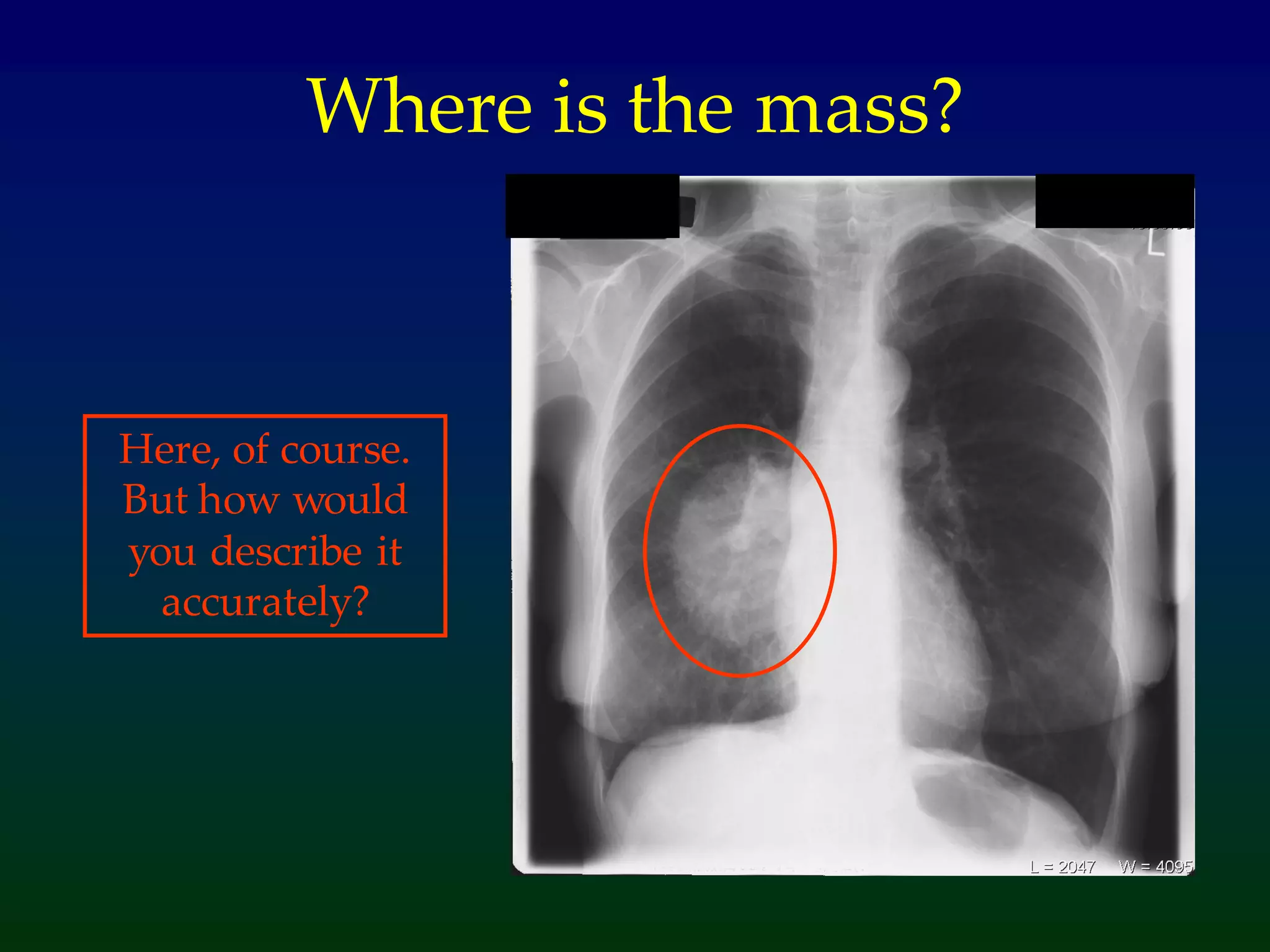
Importance of locating, describing size, and identifying features of lung masses for potential malignancy.
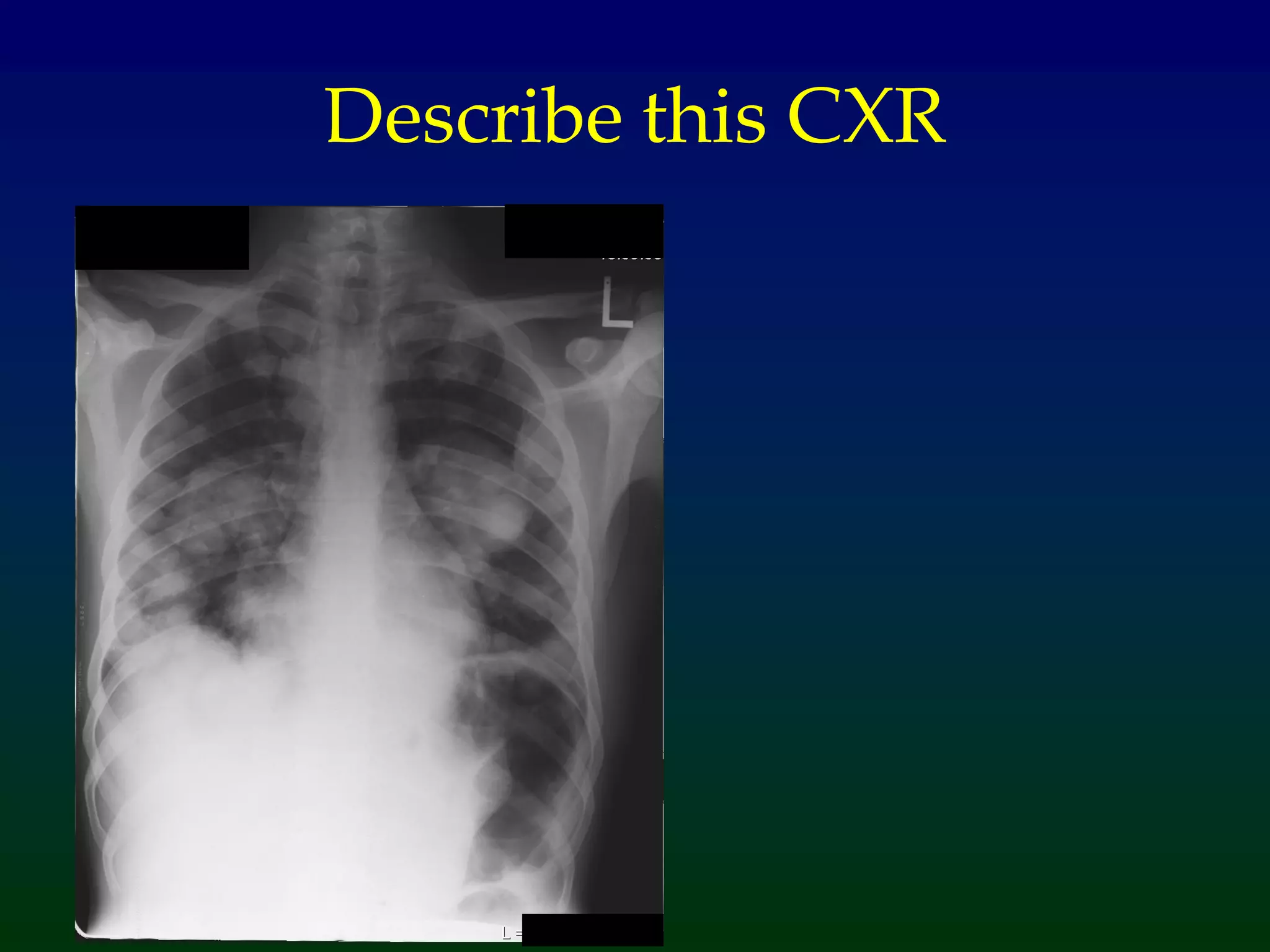
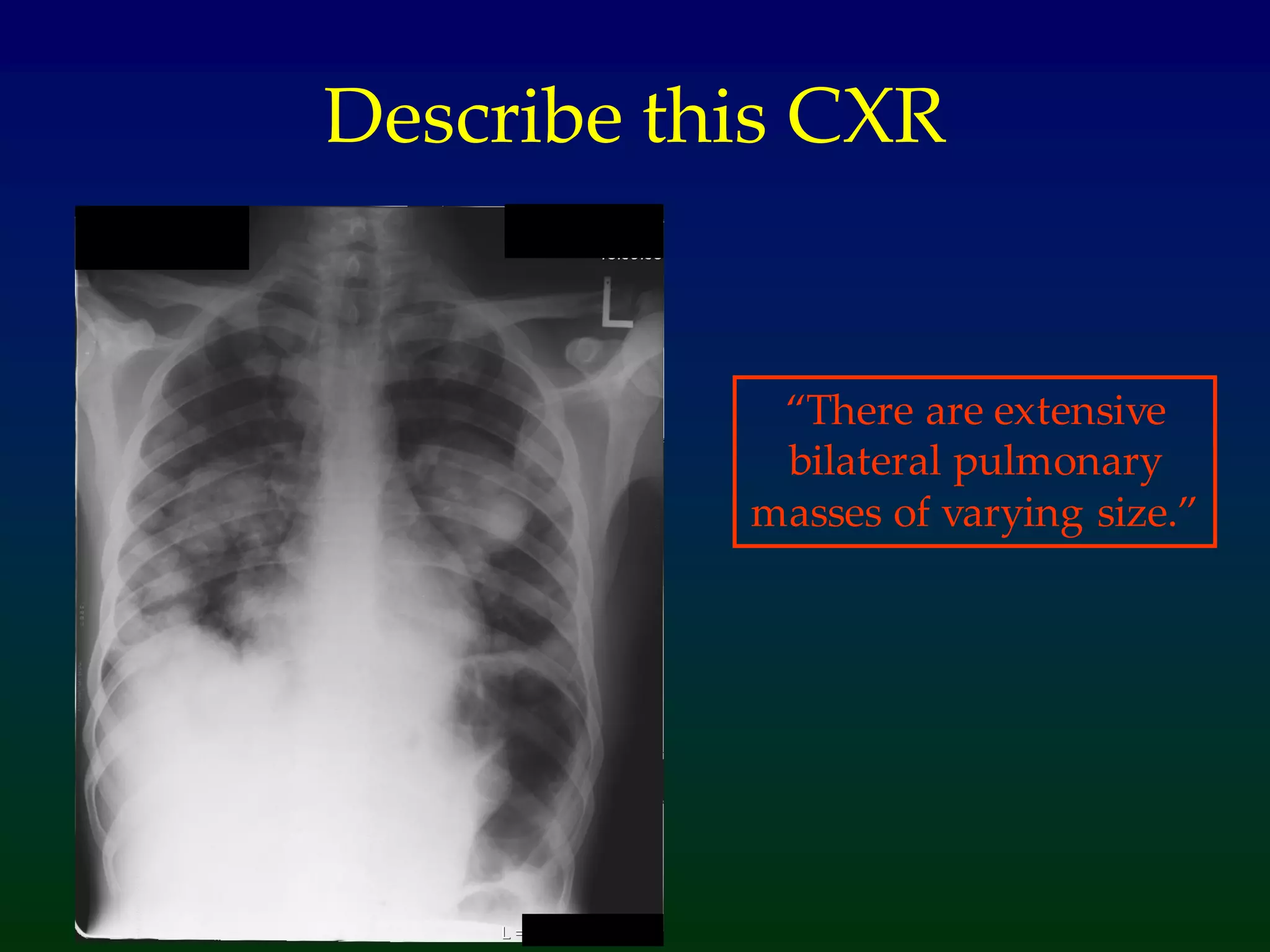
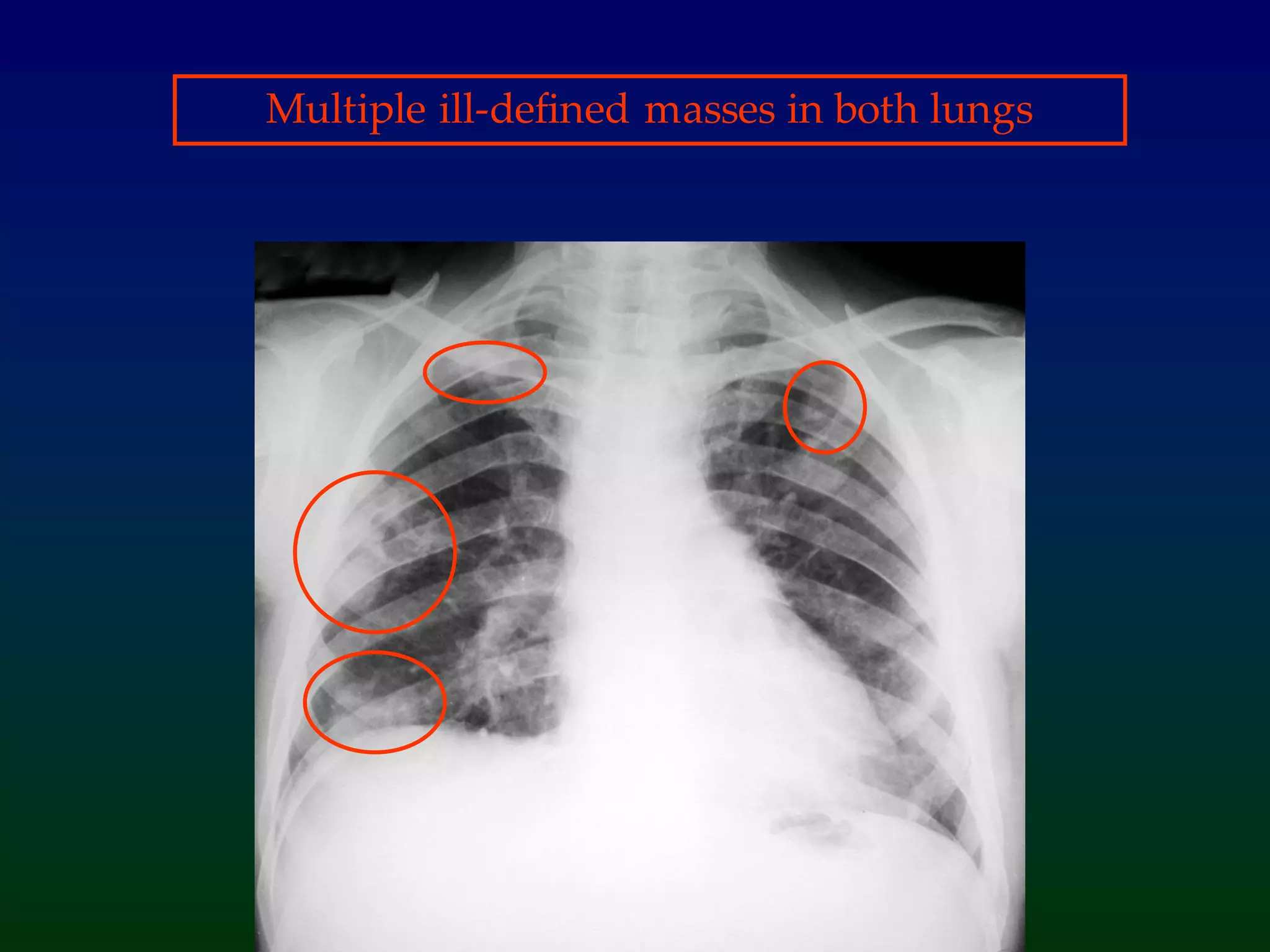
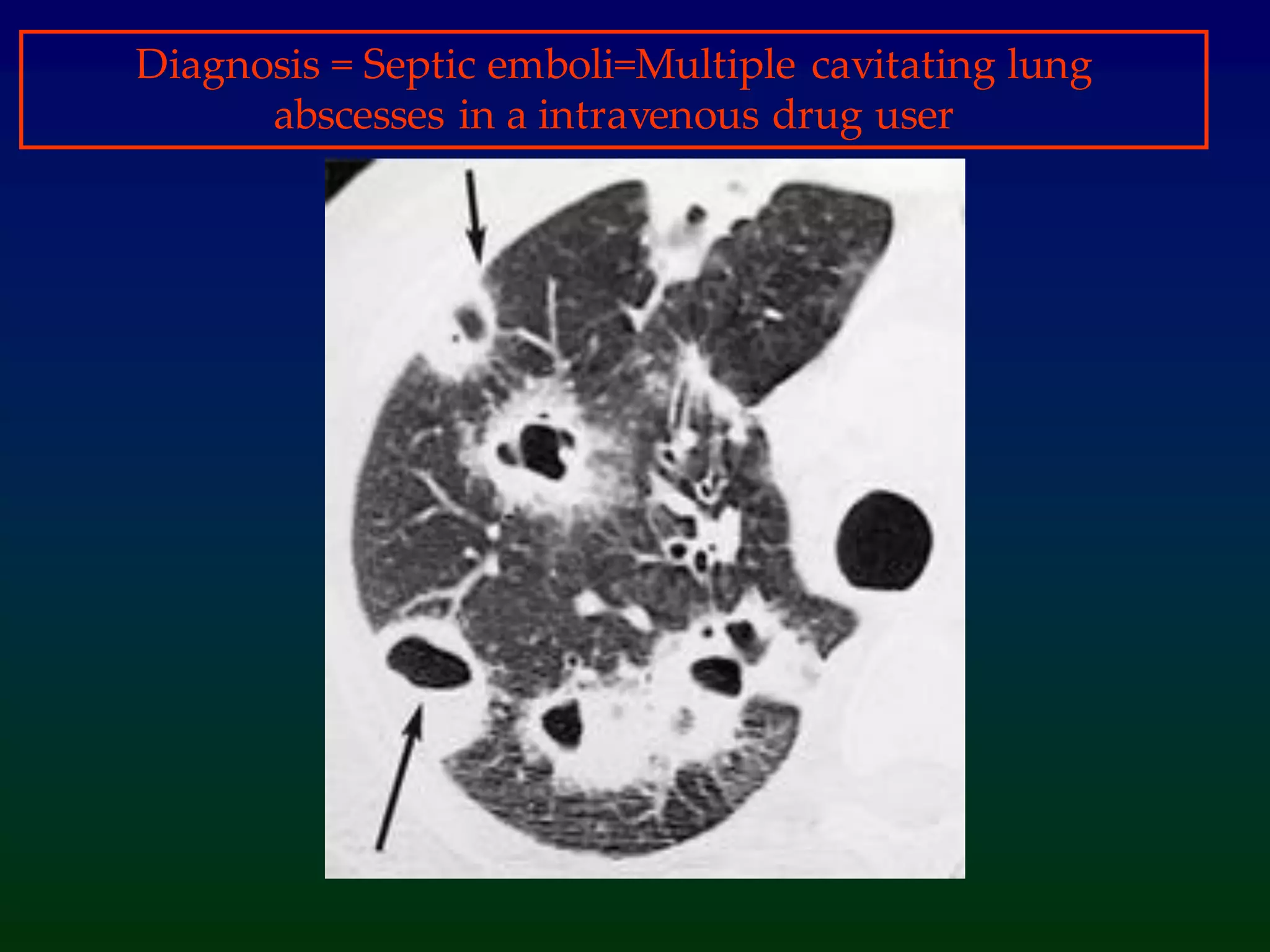
A clinical scenario involving a young male with multiple cavitating lung abscesses leading to septic emboli.
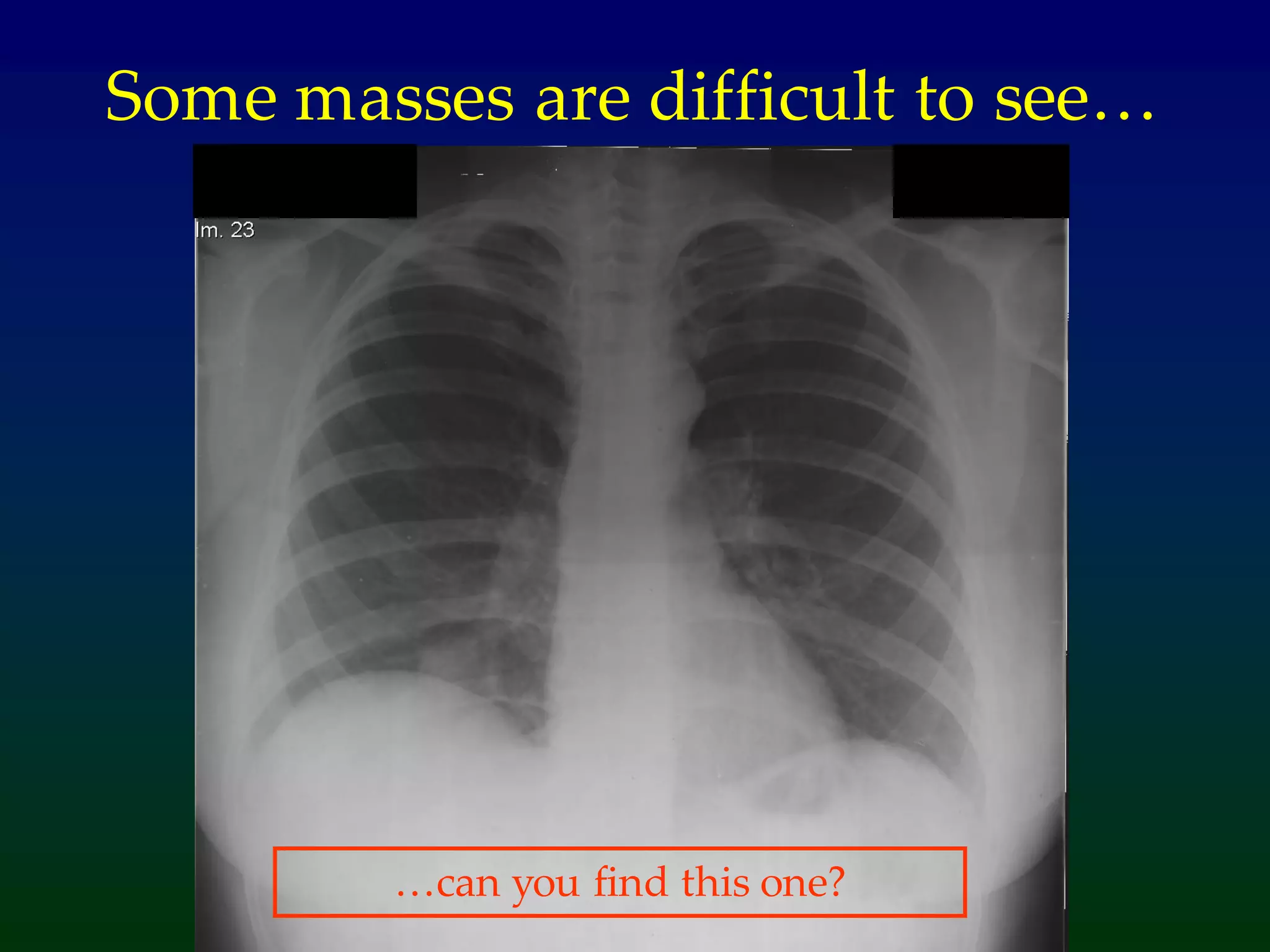
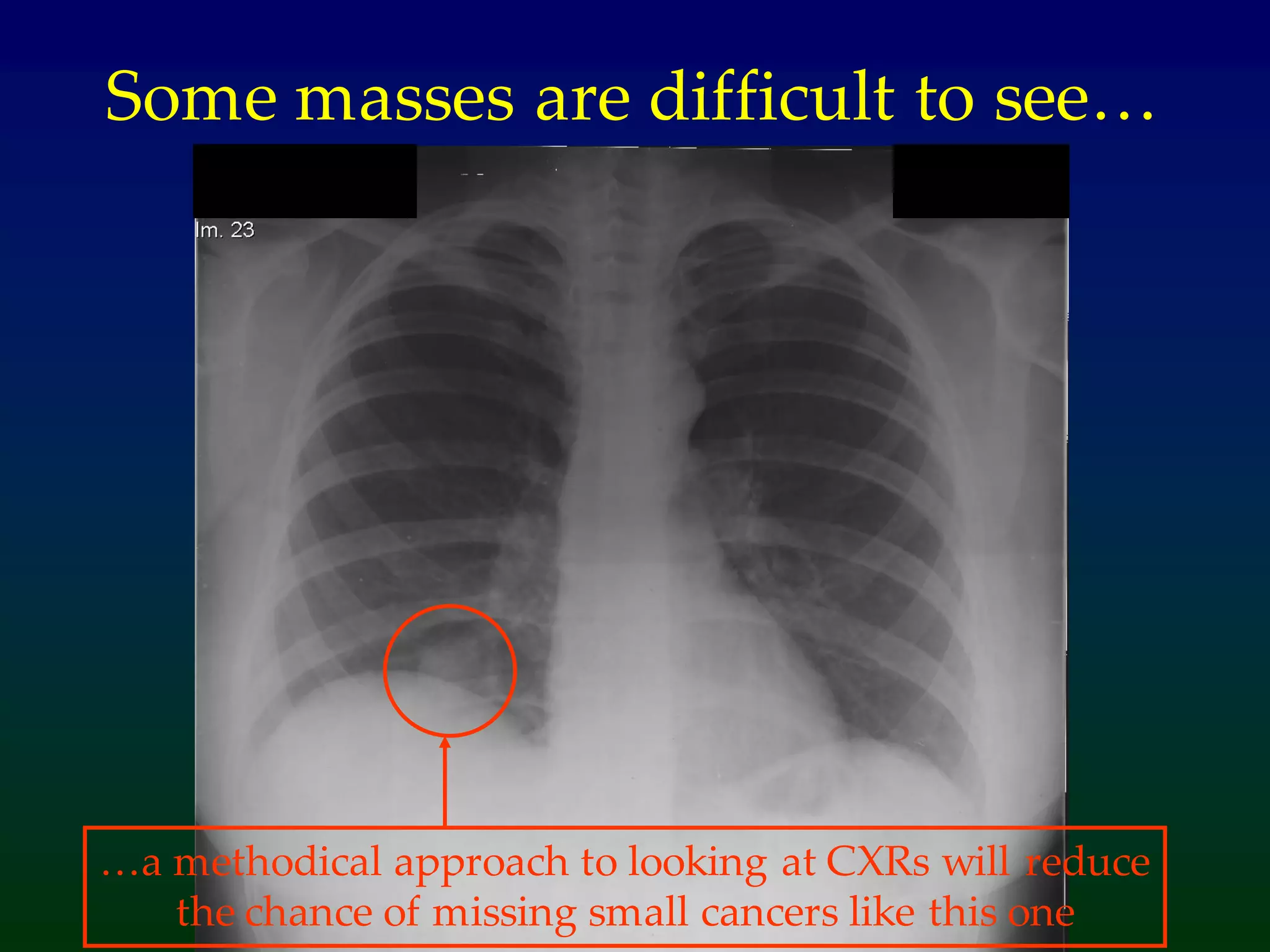
Methodical approach to identify small cancers in radiographs; emphasizes clinical history for diagnosis.
Categorization of lung cancer types: Small Cell (20-25%) and Non-Small Cell Lung Cancer (80%).
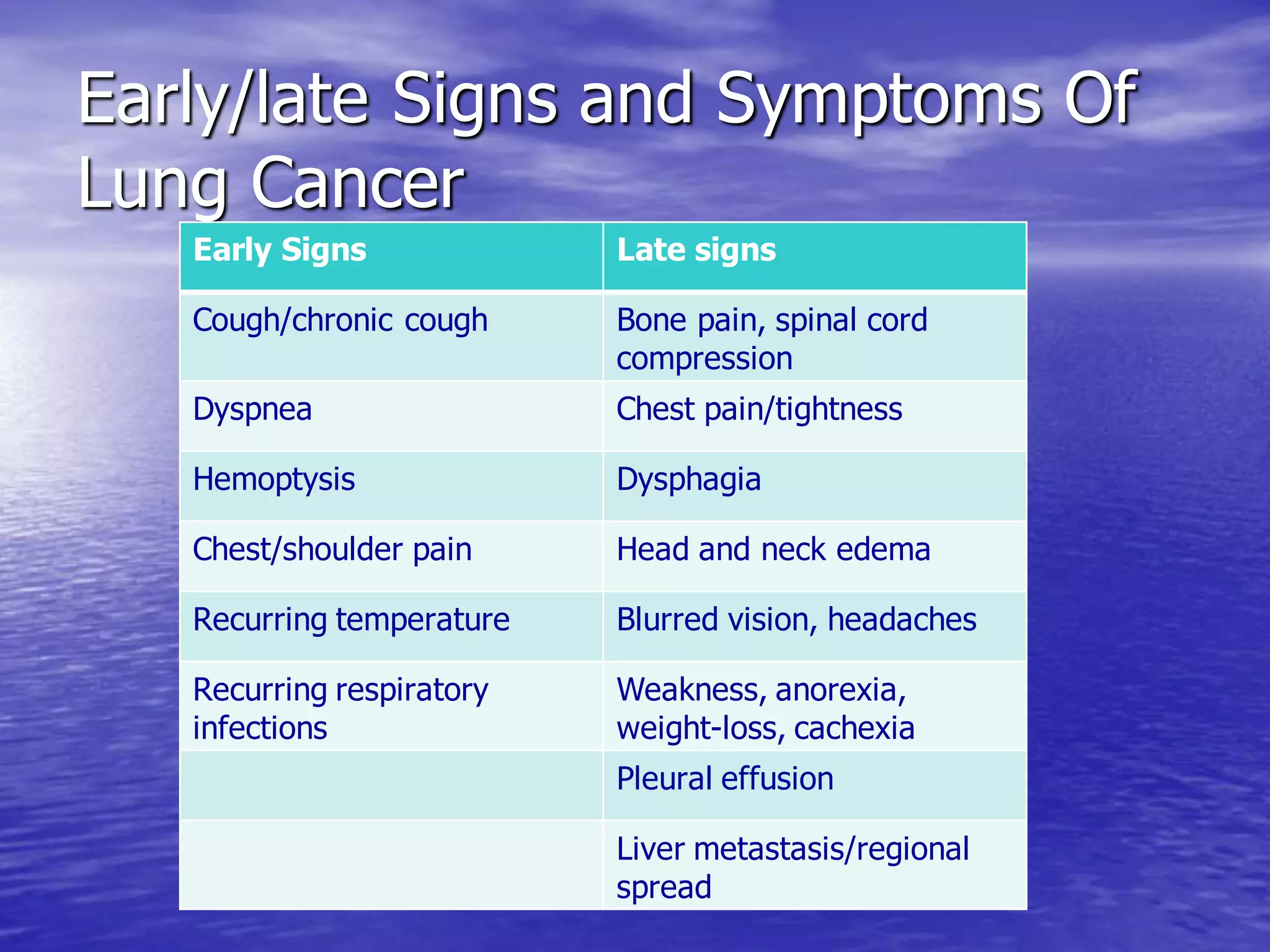
Discussion on causes, risk factors, early and late signs of lung cancer, including diverse symptoms.
Various diagnostic tests like CXR, CT Scans, and biopsies, focusing on their role in identifying lung cancer.
Potential post-operative complications arising post lung cancer surgery, including respiratory failure.
Various treatment modalities: surgery, radiation therapy, and chemotherapy, along with their types.
Introduction to complementary therapies like acupuncture and herbal medicine which may aid lung cancer treatment.
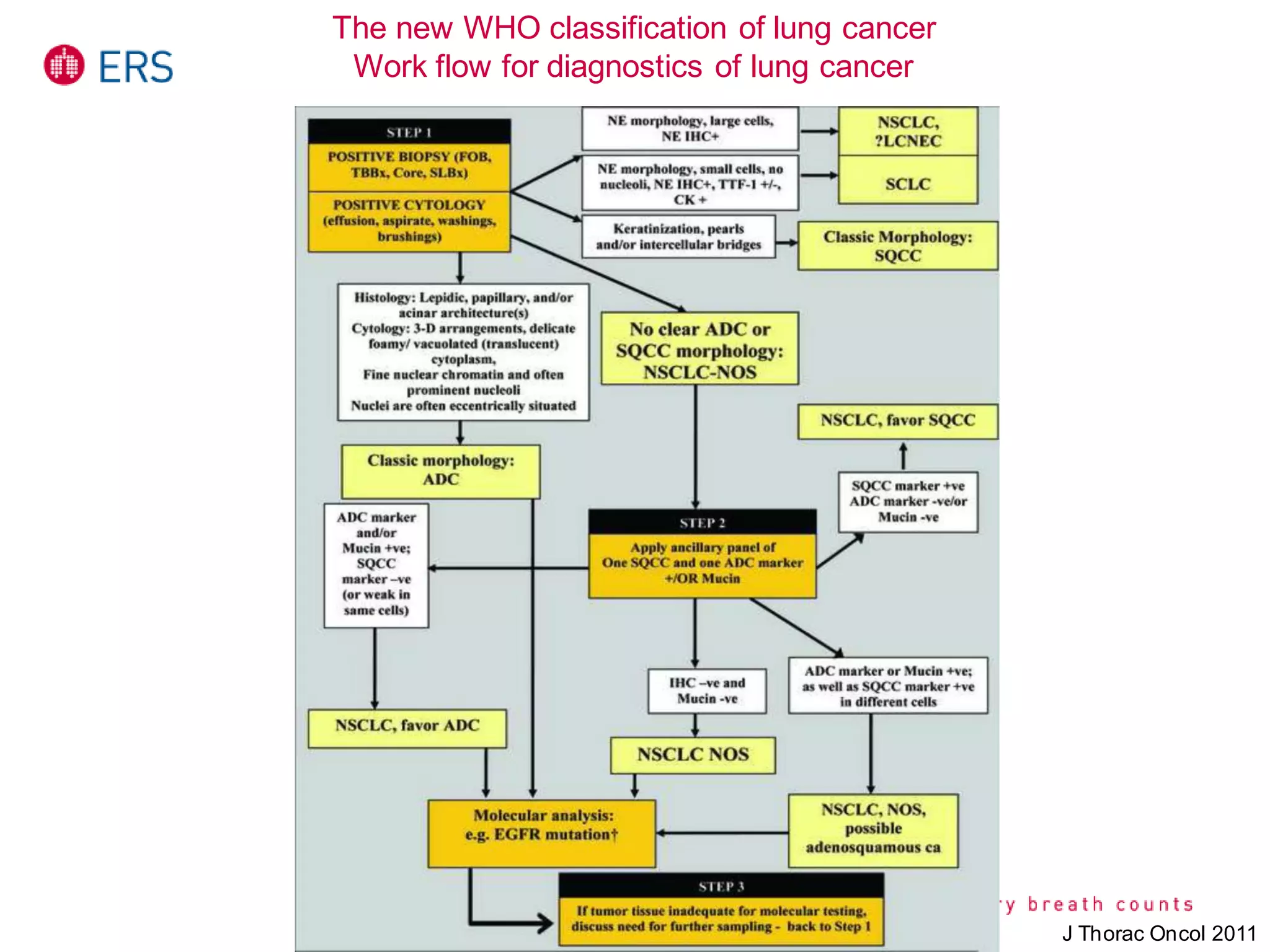
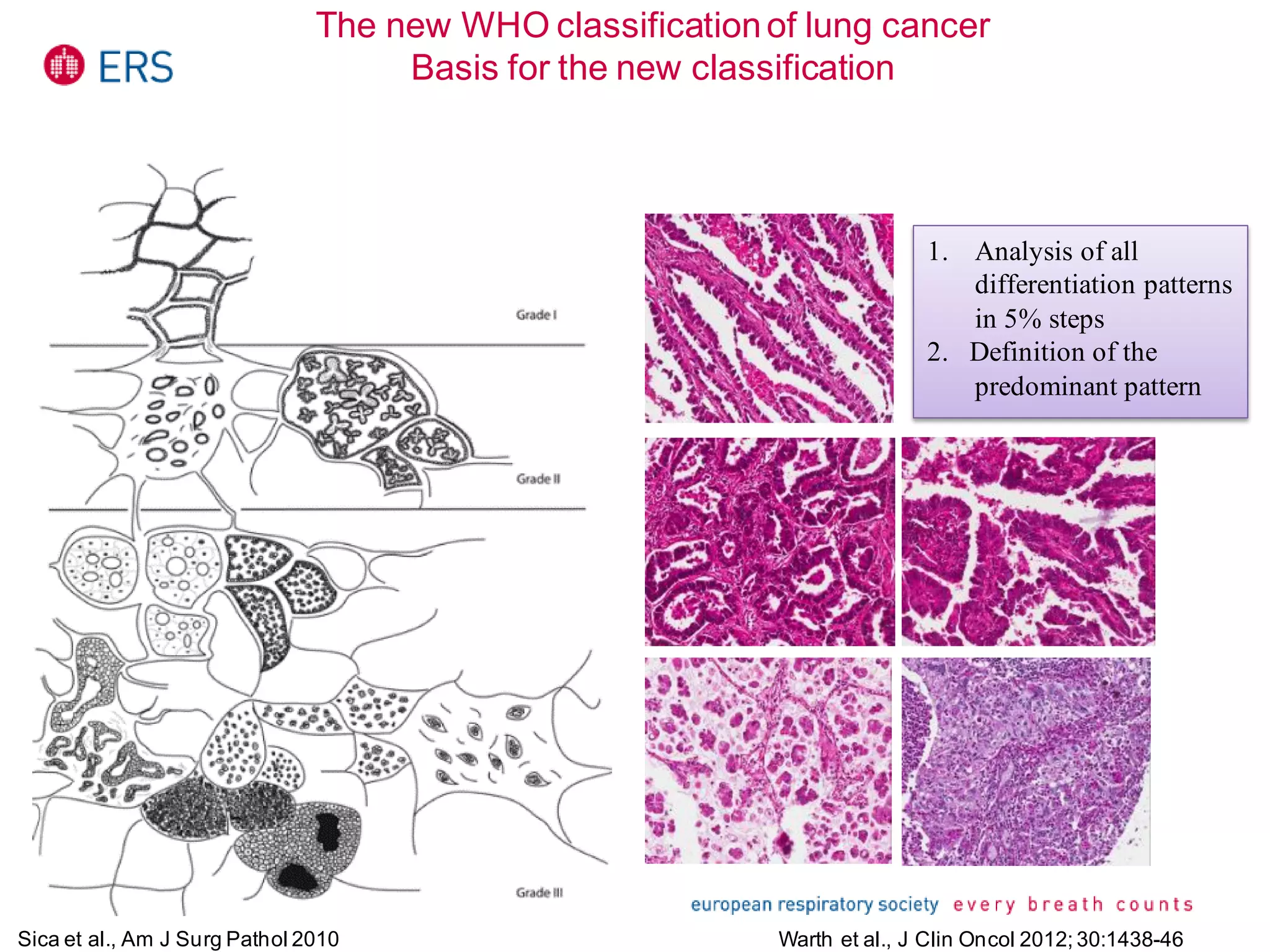
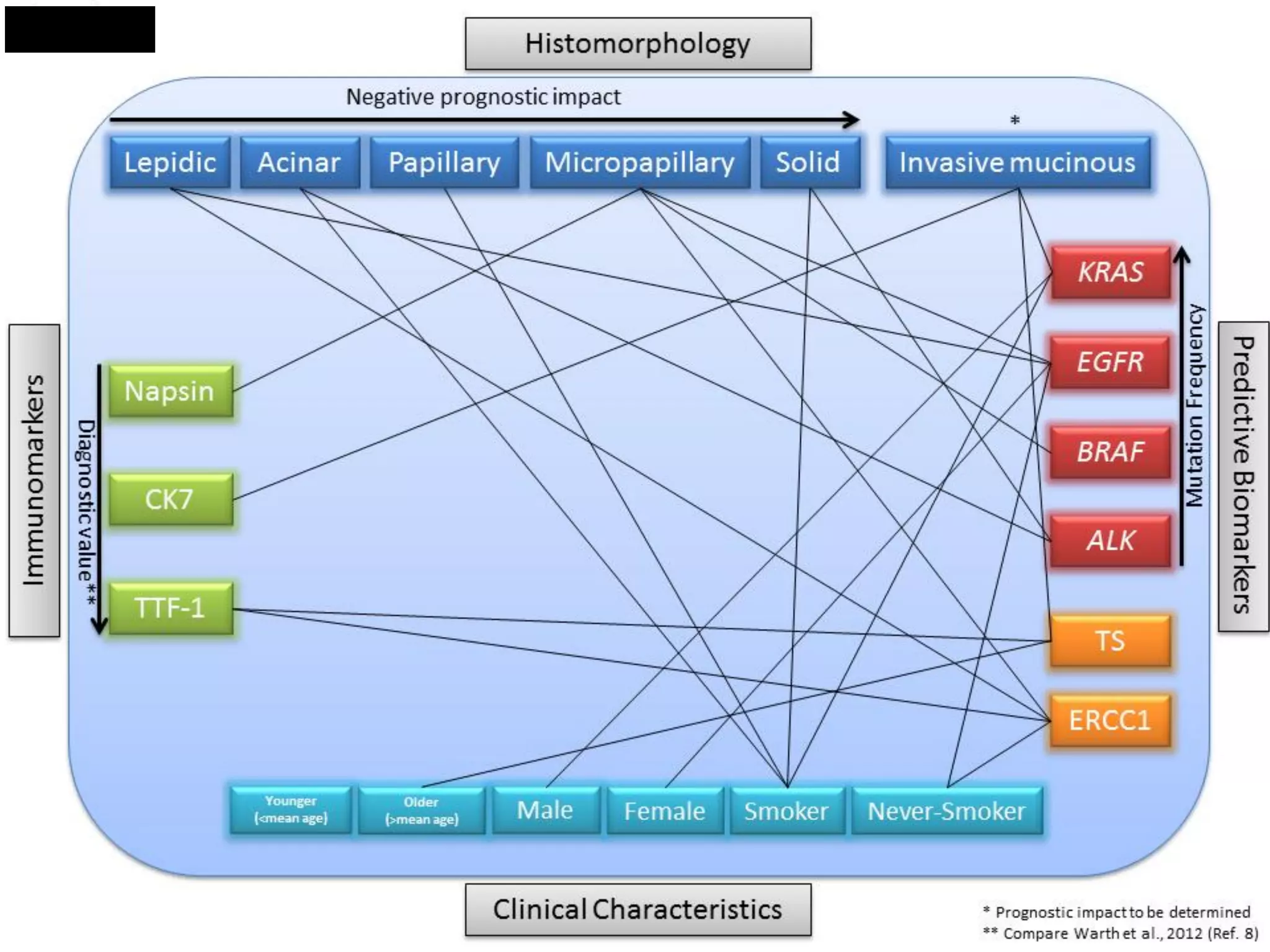
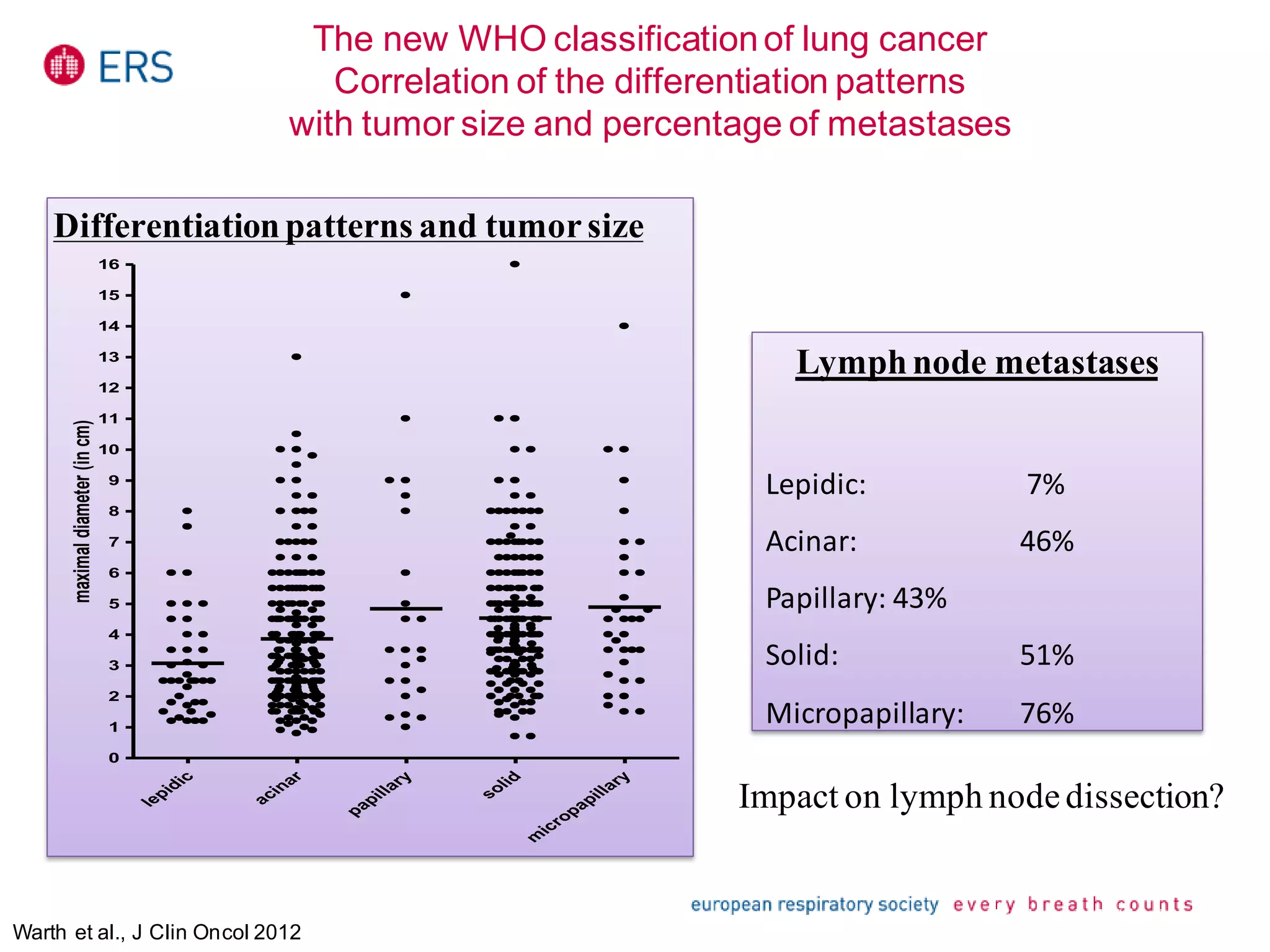
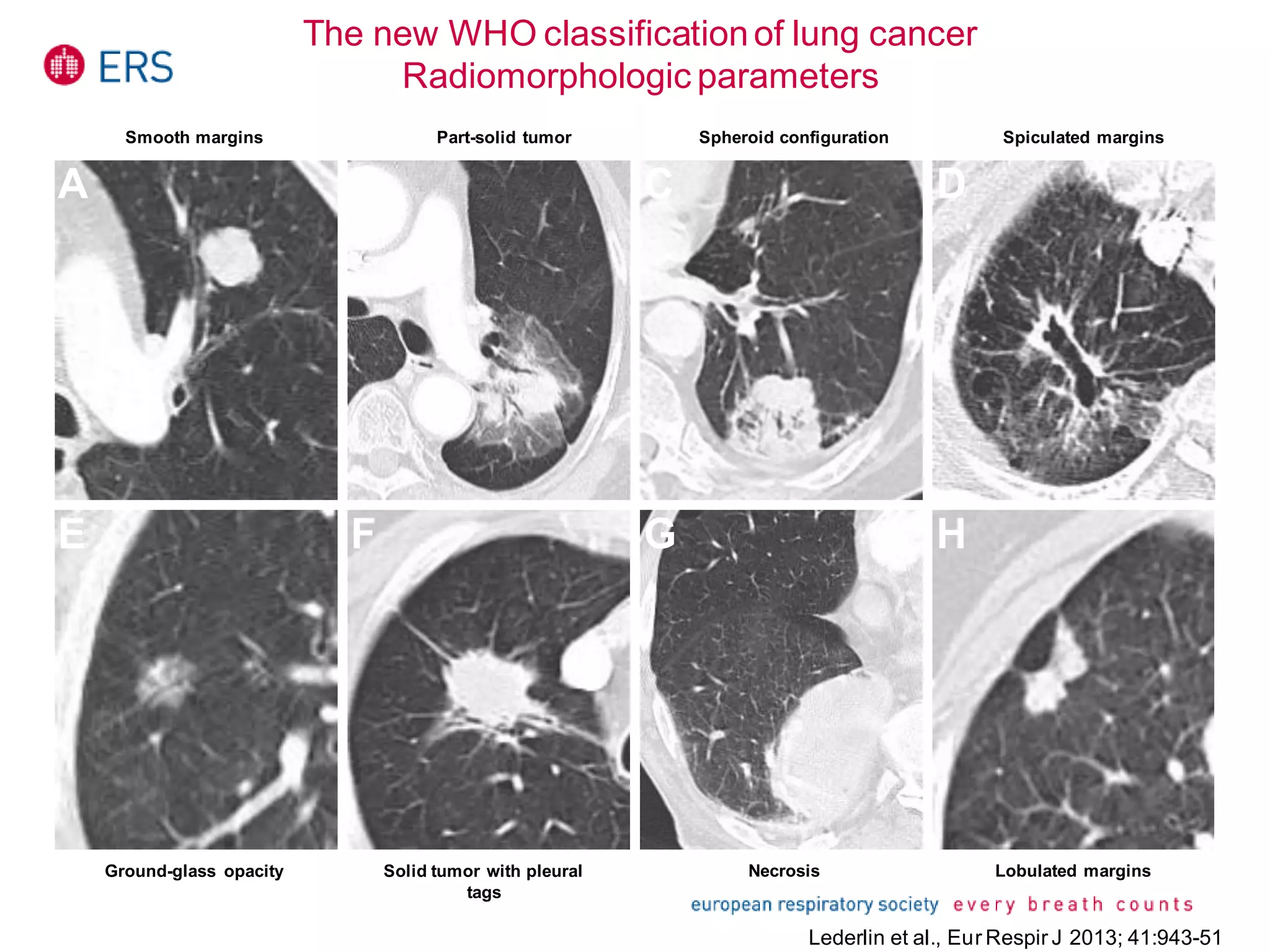
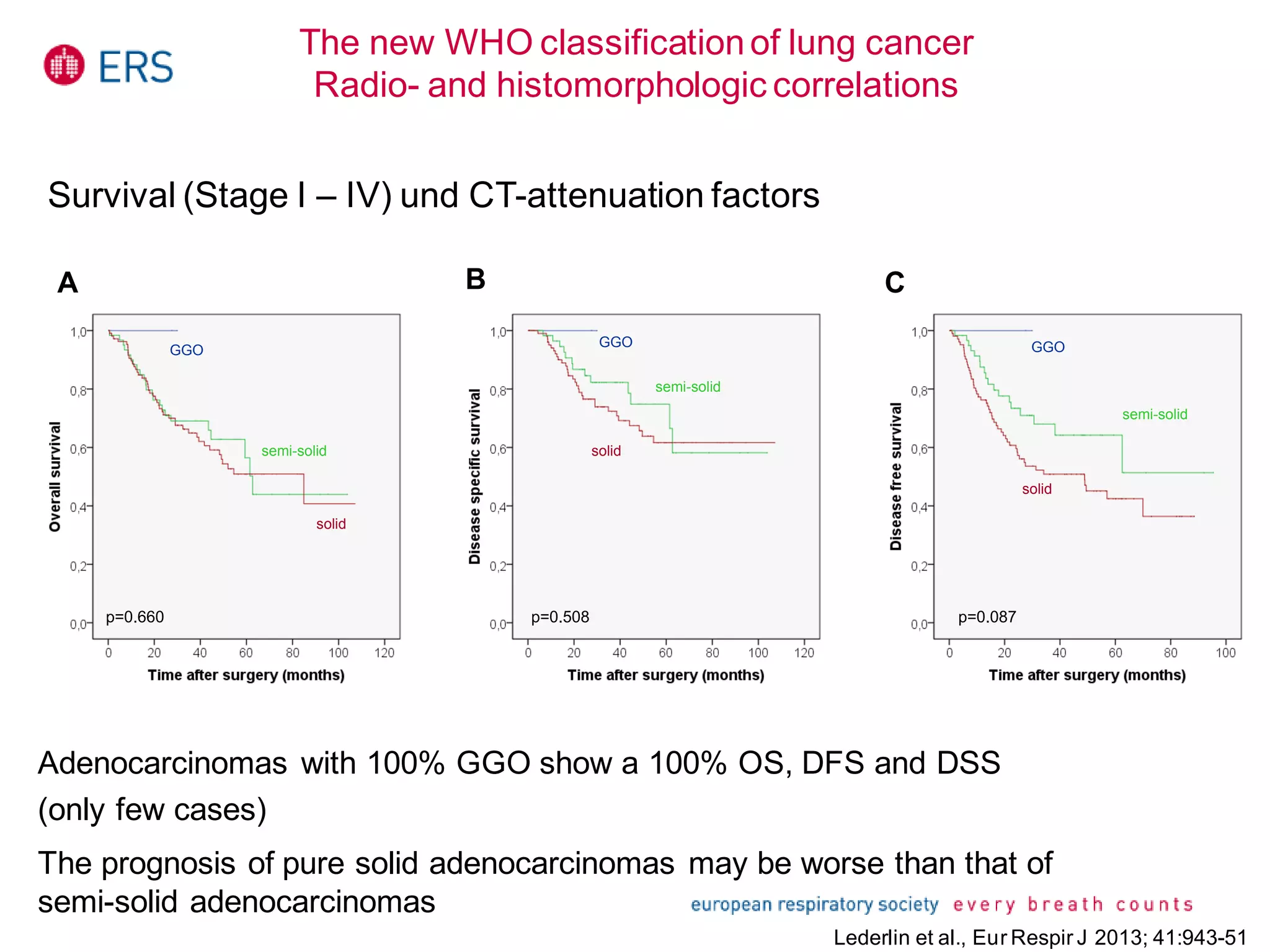
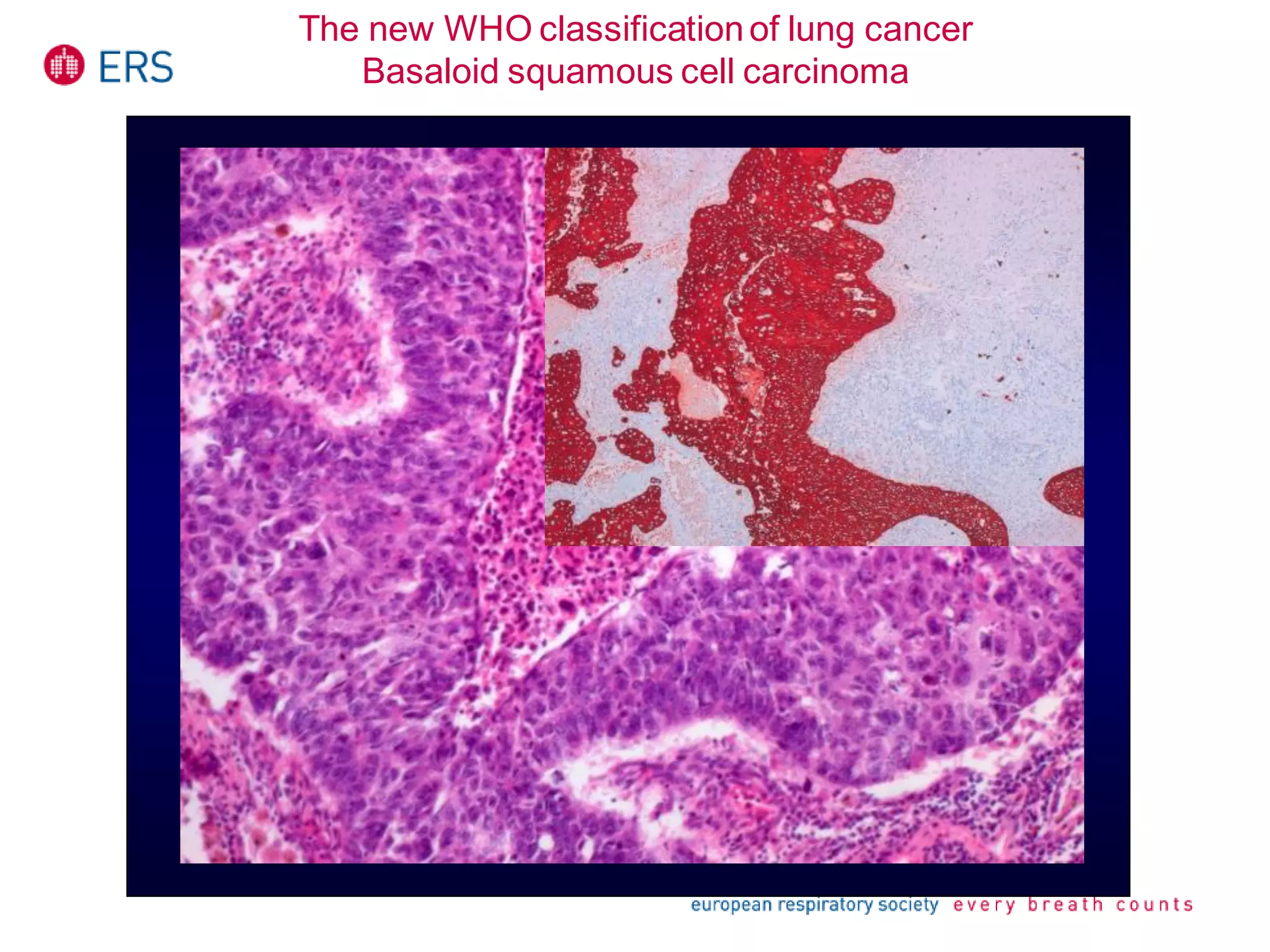
New classifications based on histopathology, diagnostic criteria improvements and various tumor types.
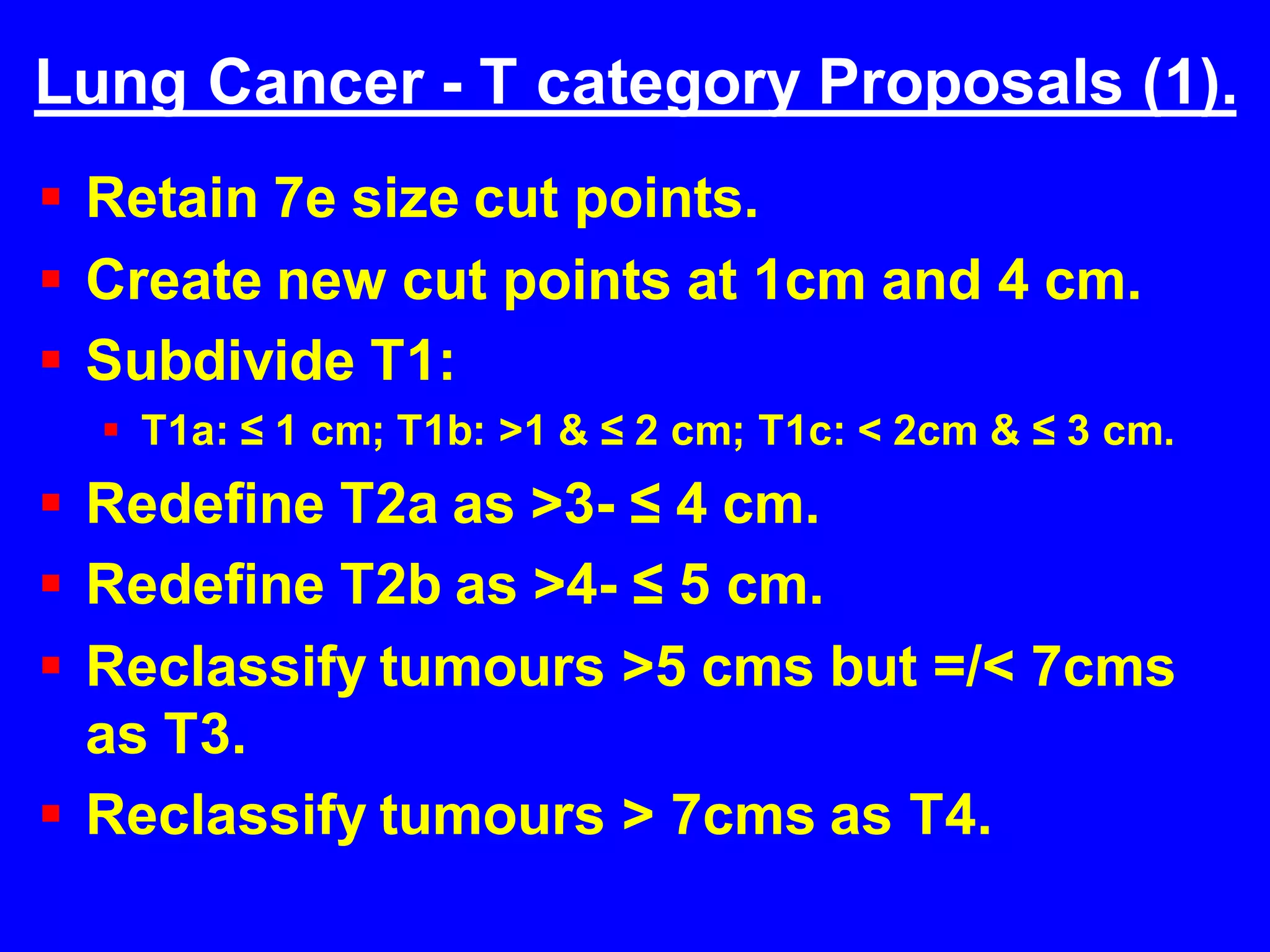
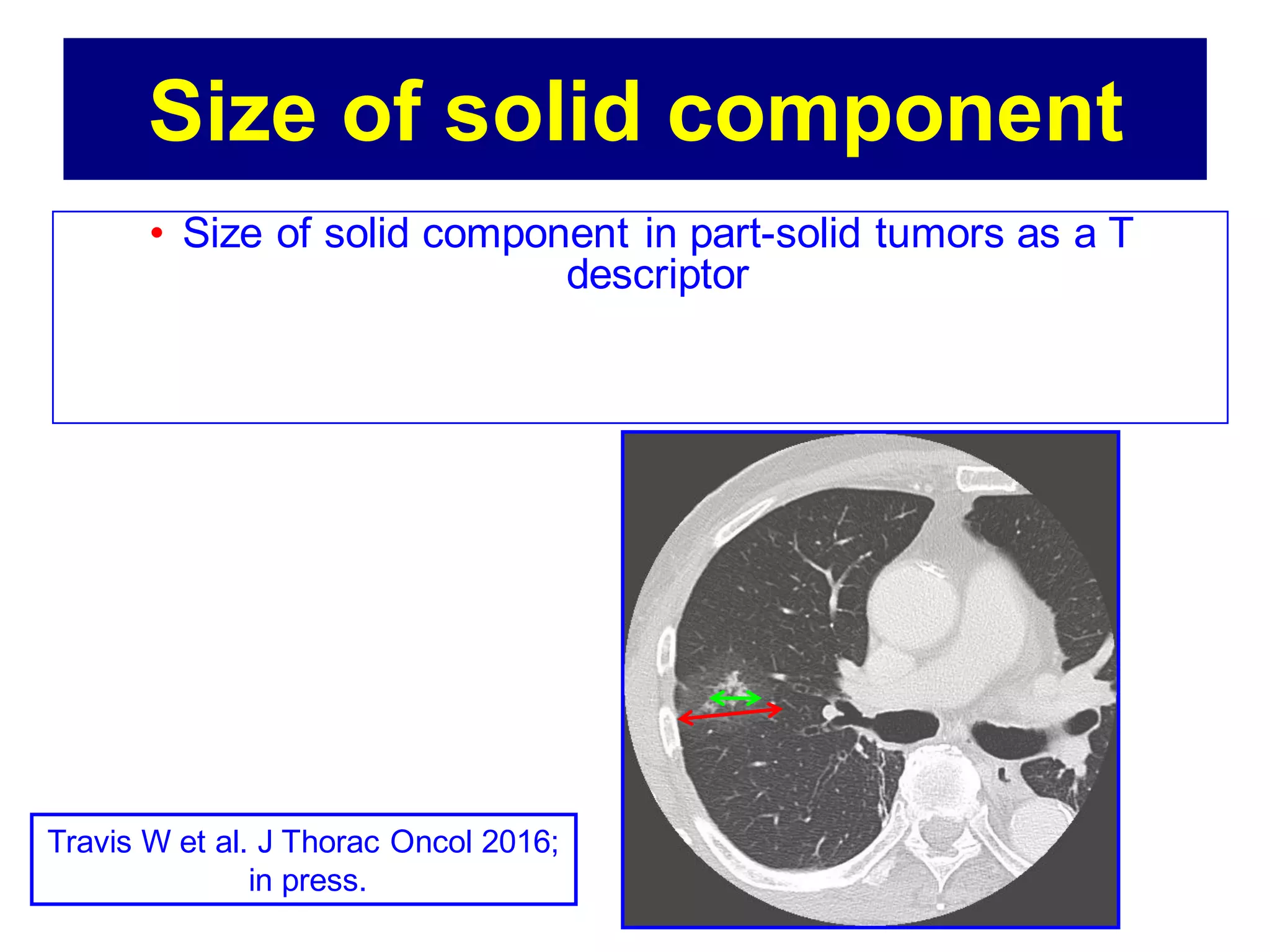
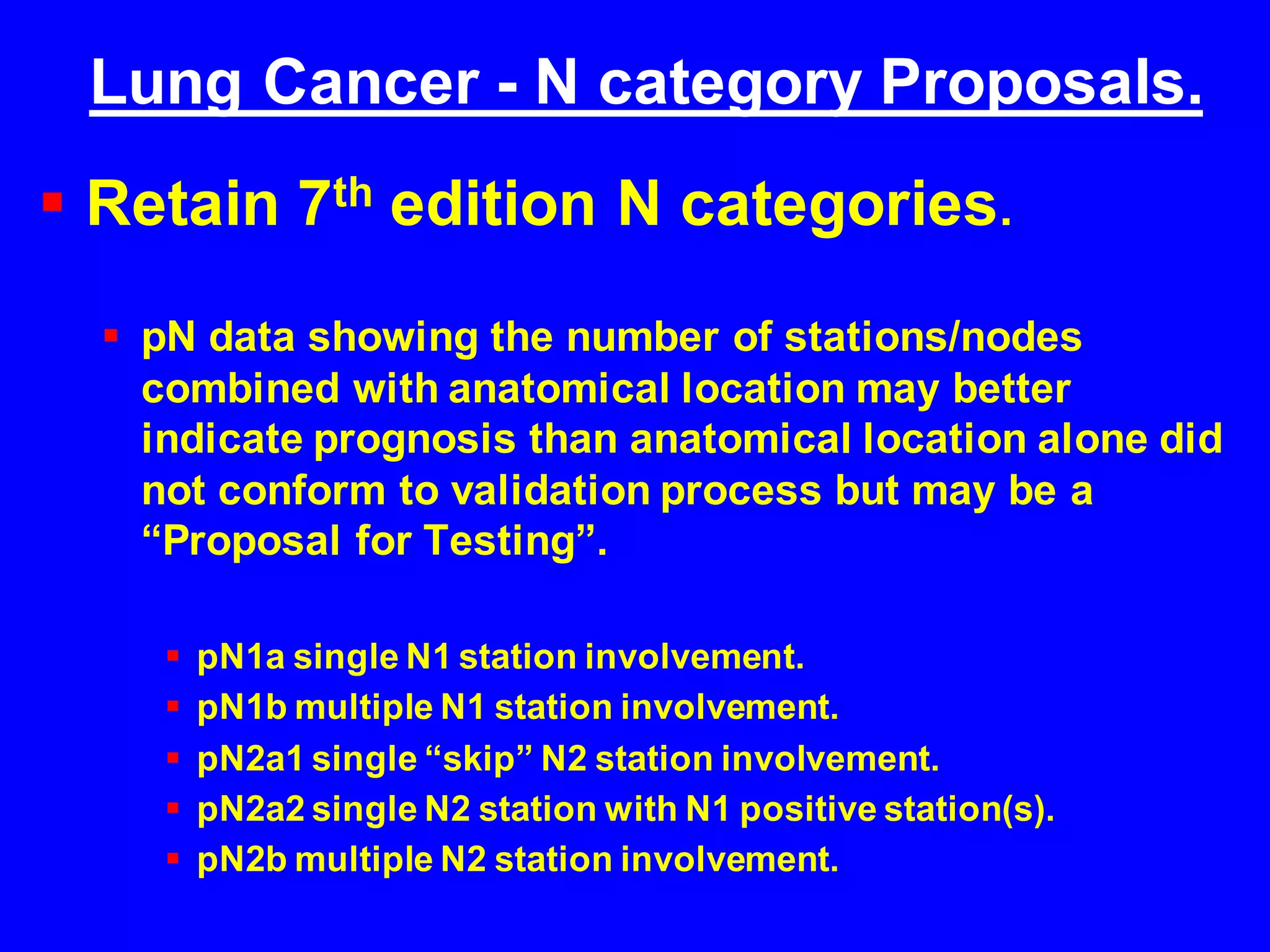
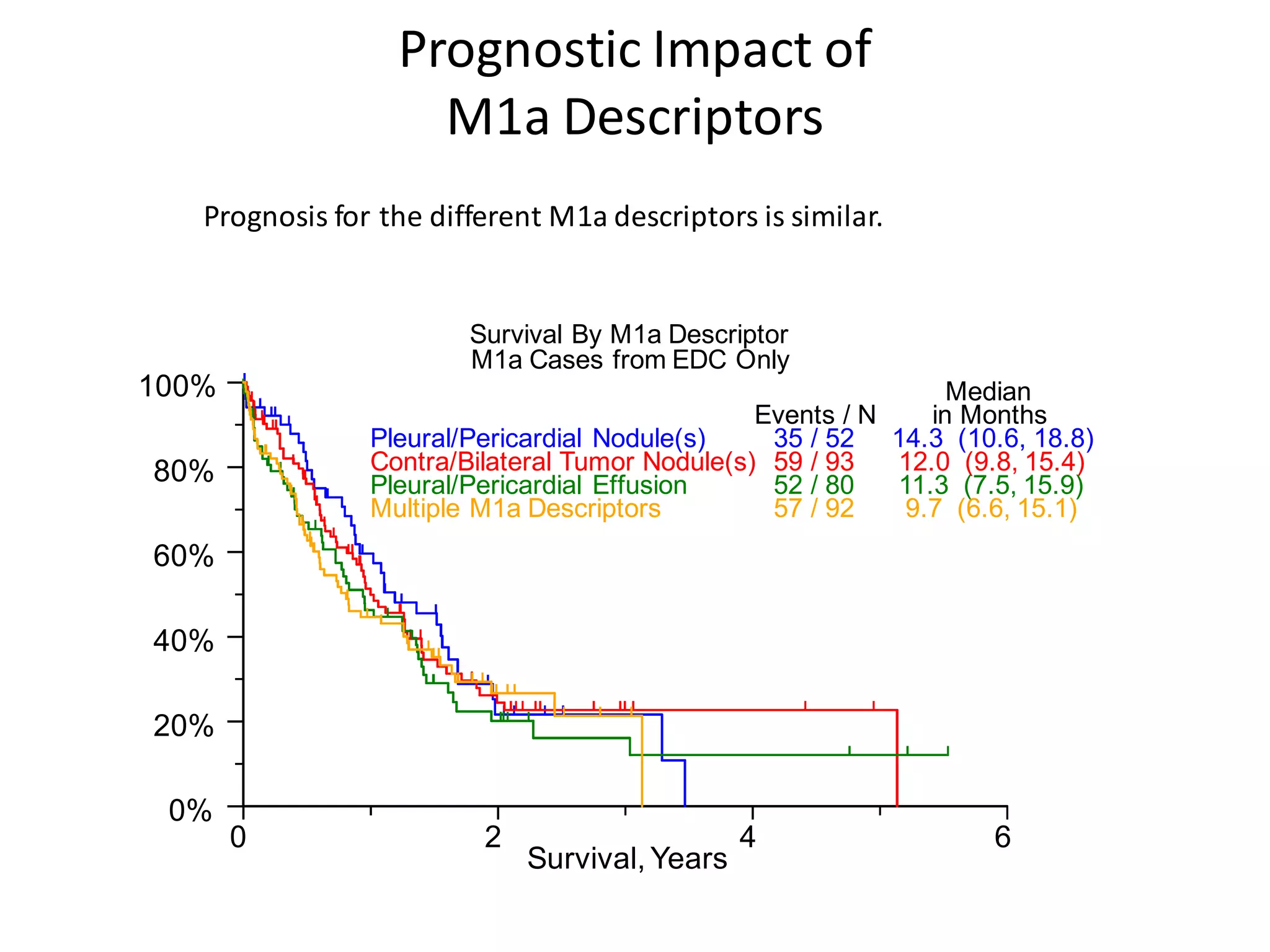
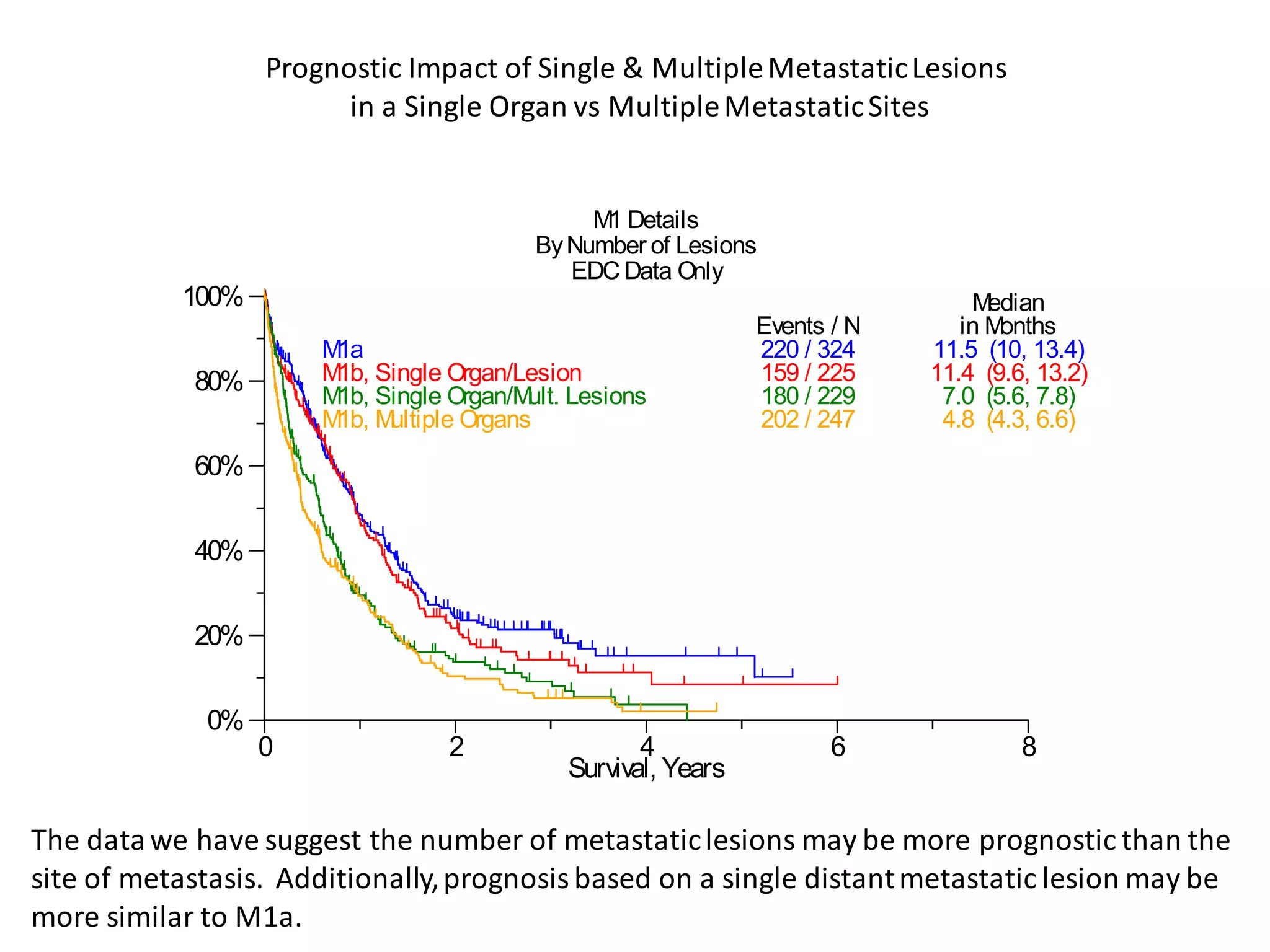
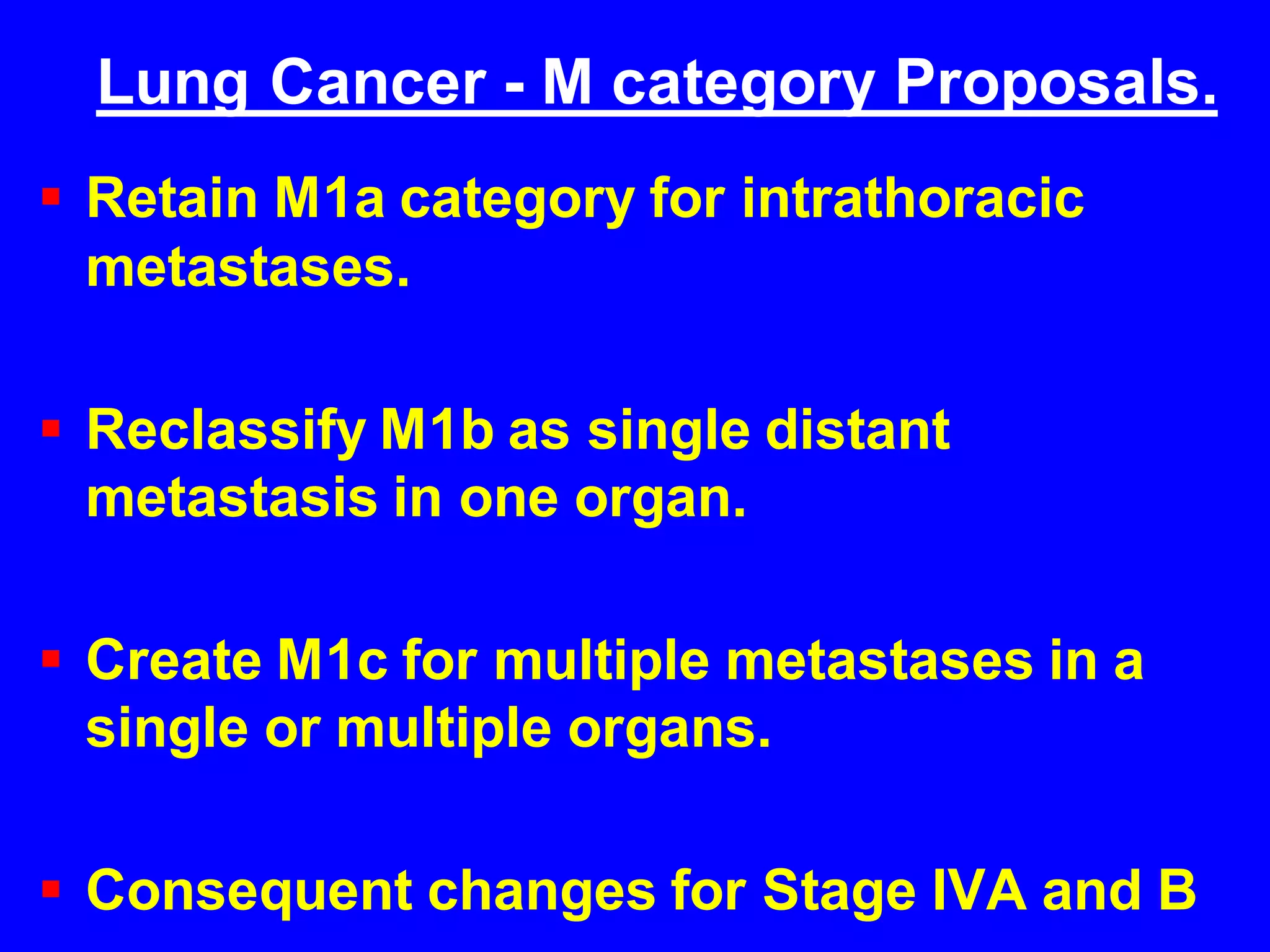
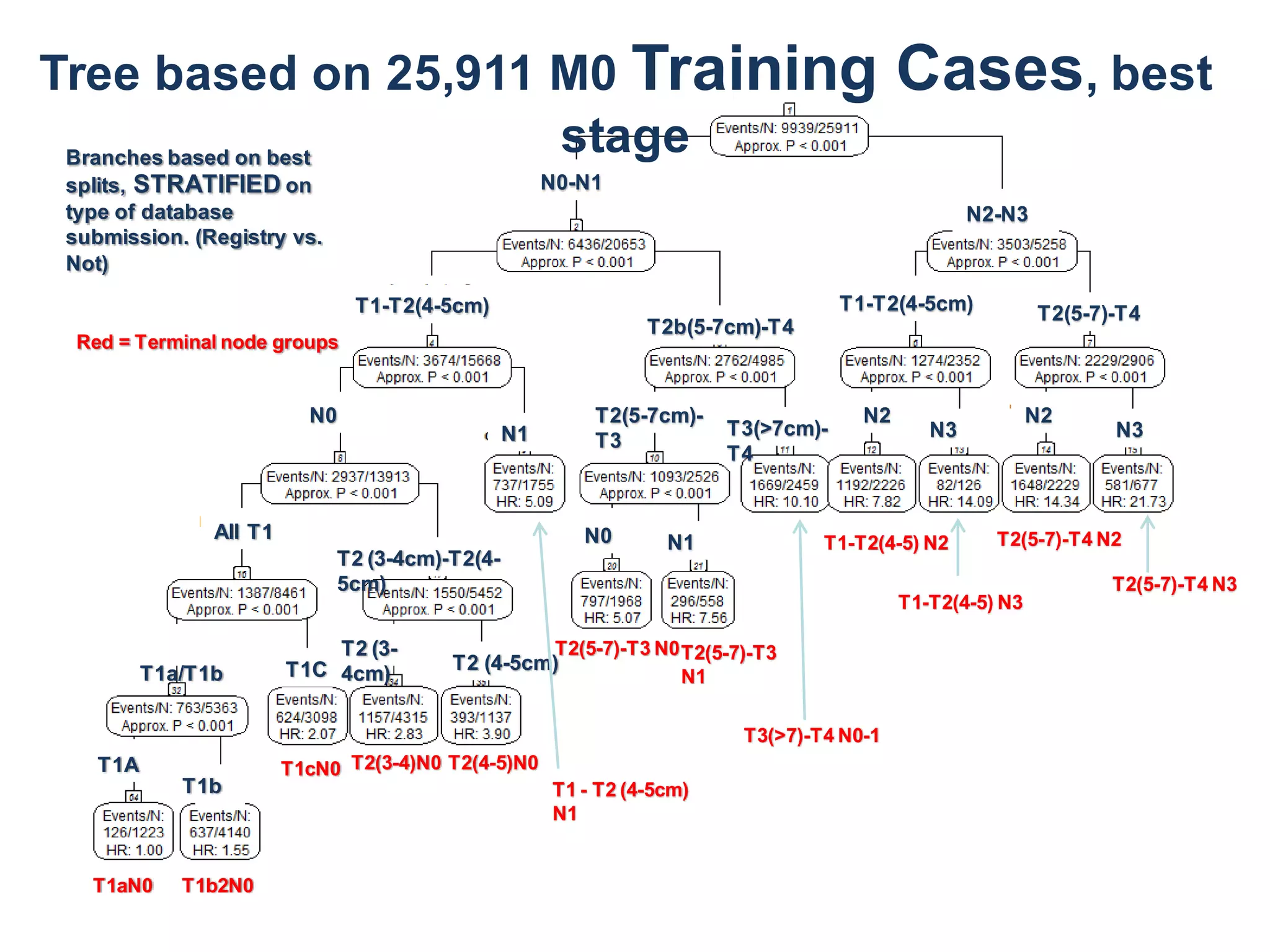
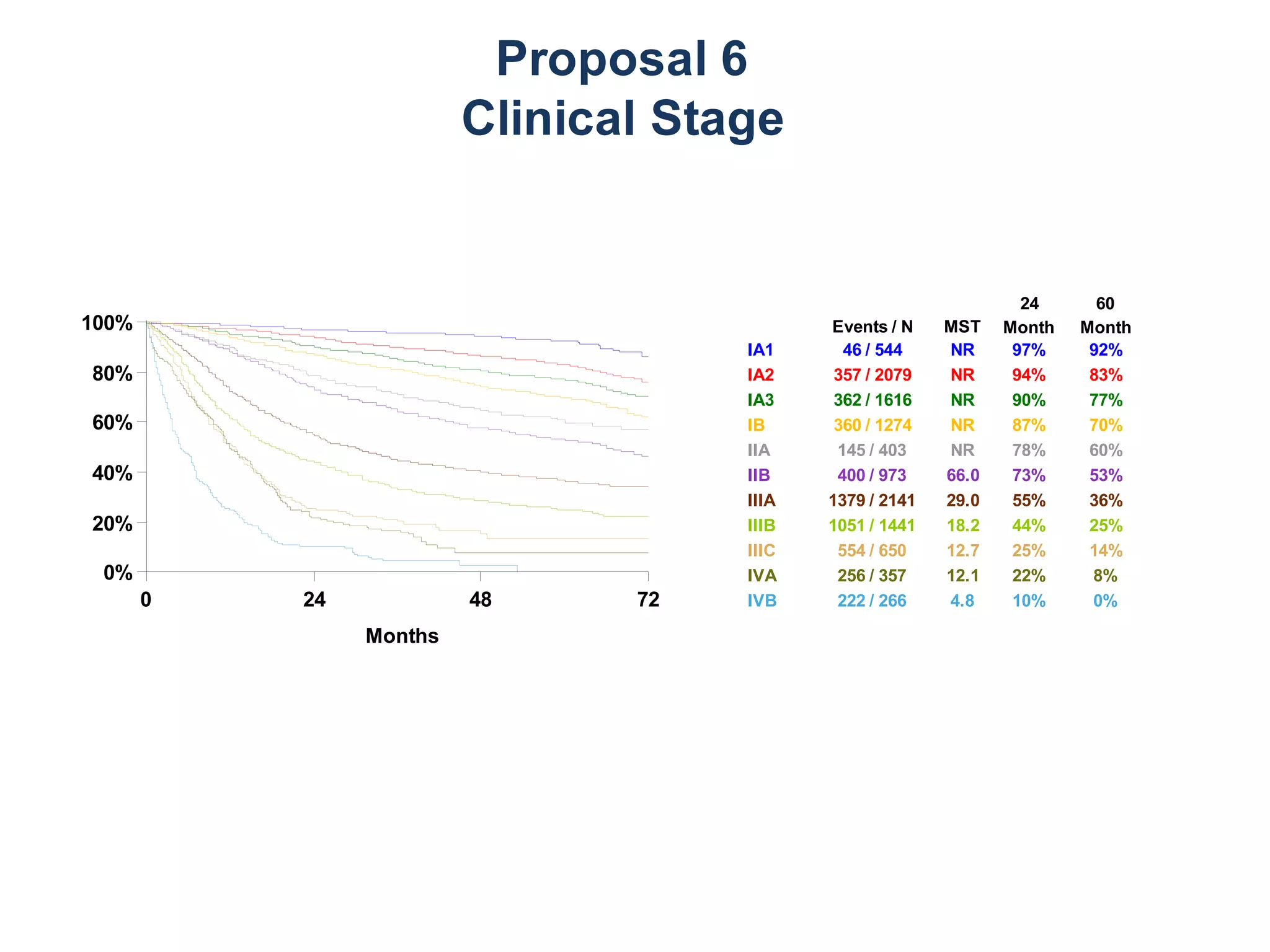
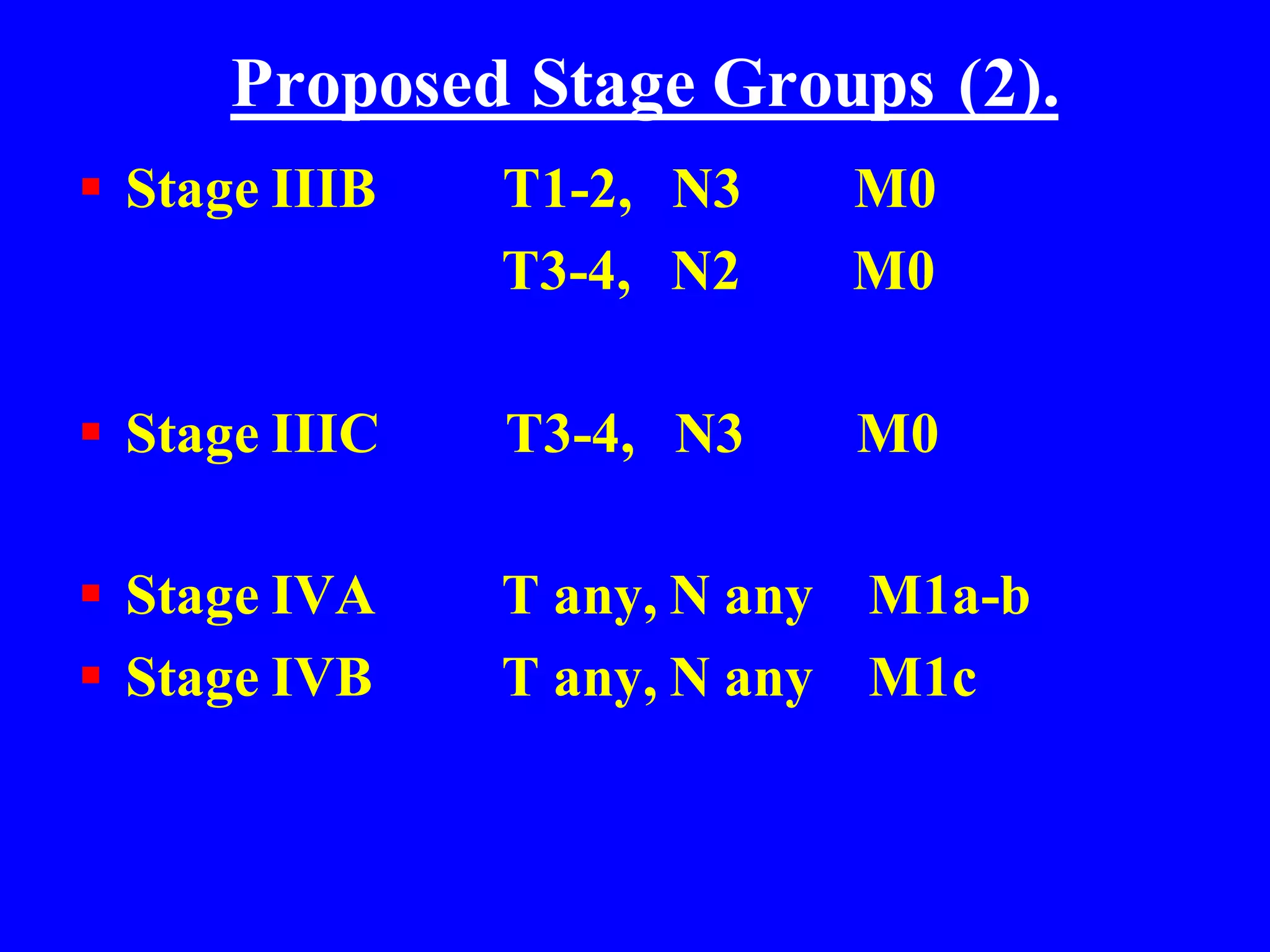
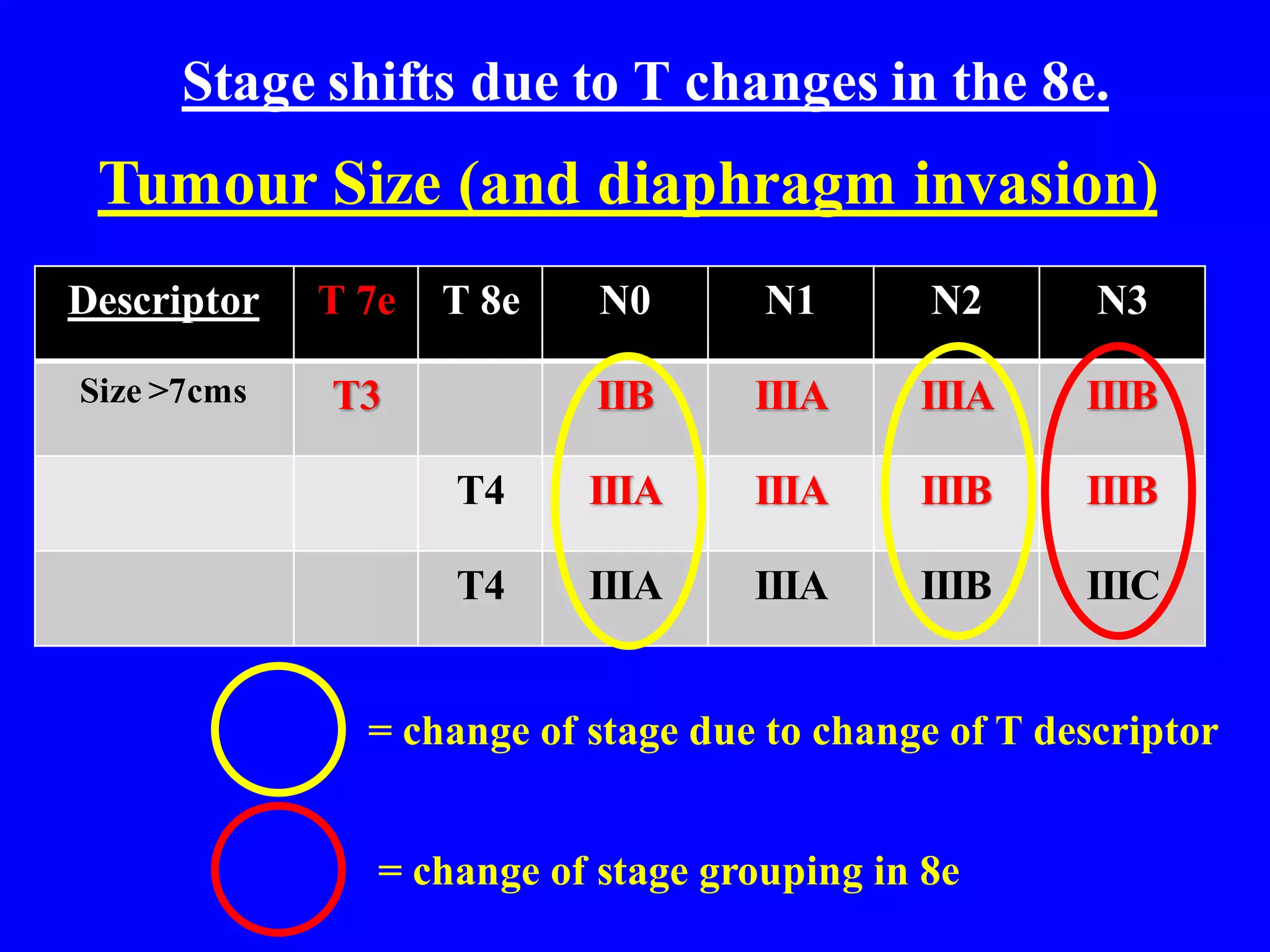
New TNM staging guidelines for lung cancer, detailing criteria for determining prognosis and treatment direction.
Recommendations for managing lung cancer, focusing on case studies and predictors of malignancy.
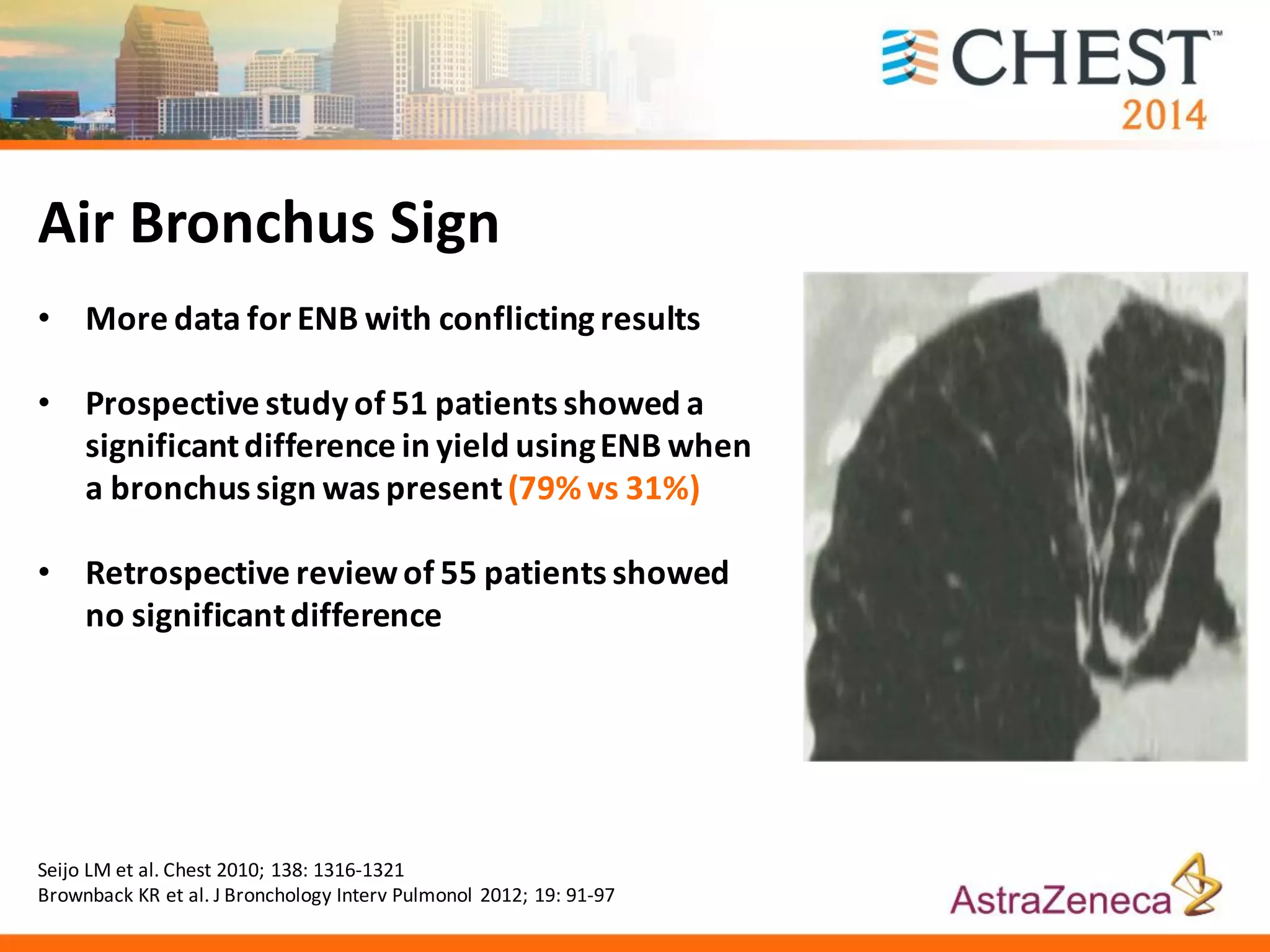
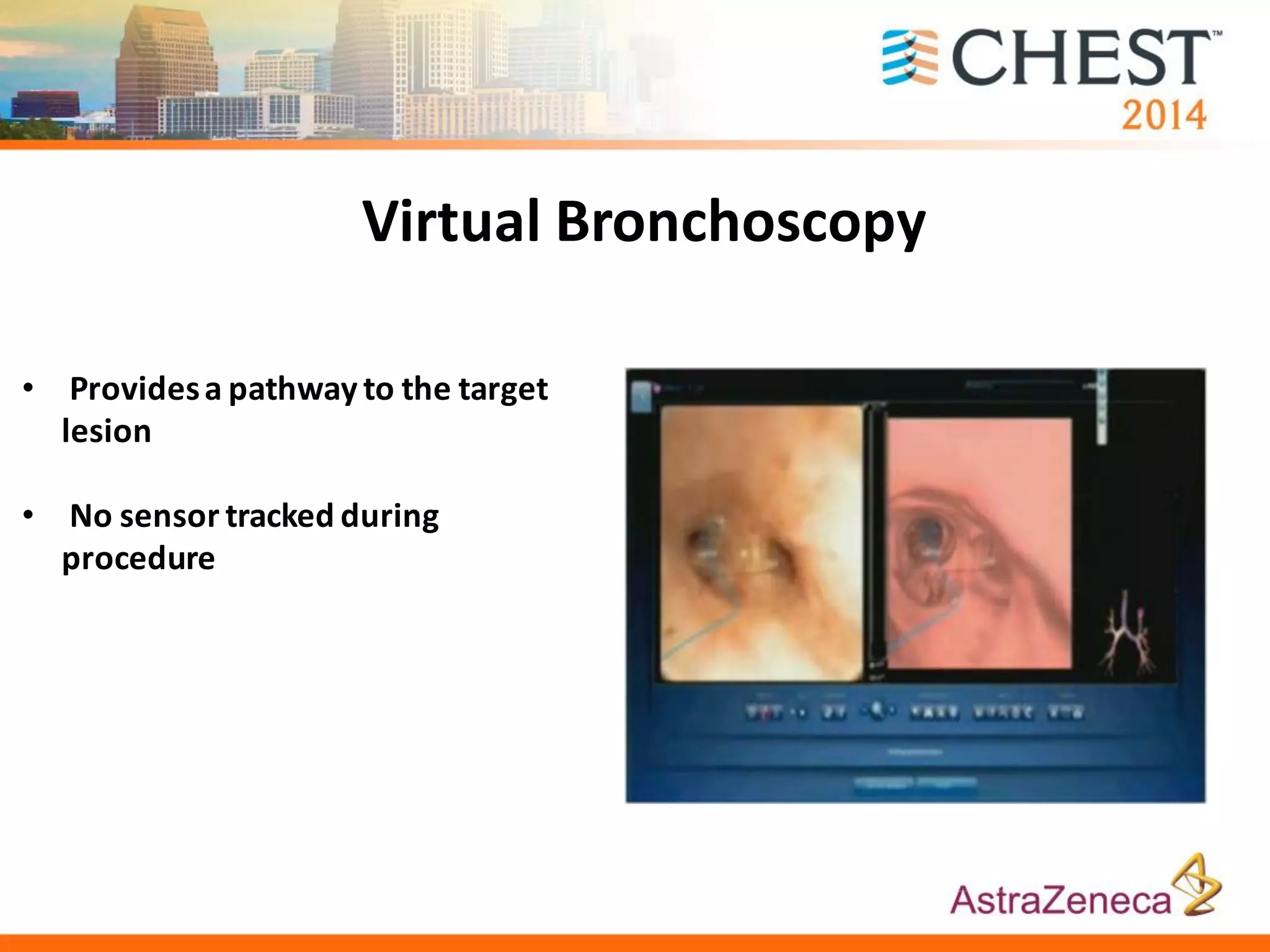
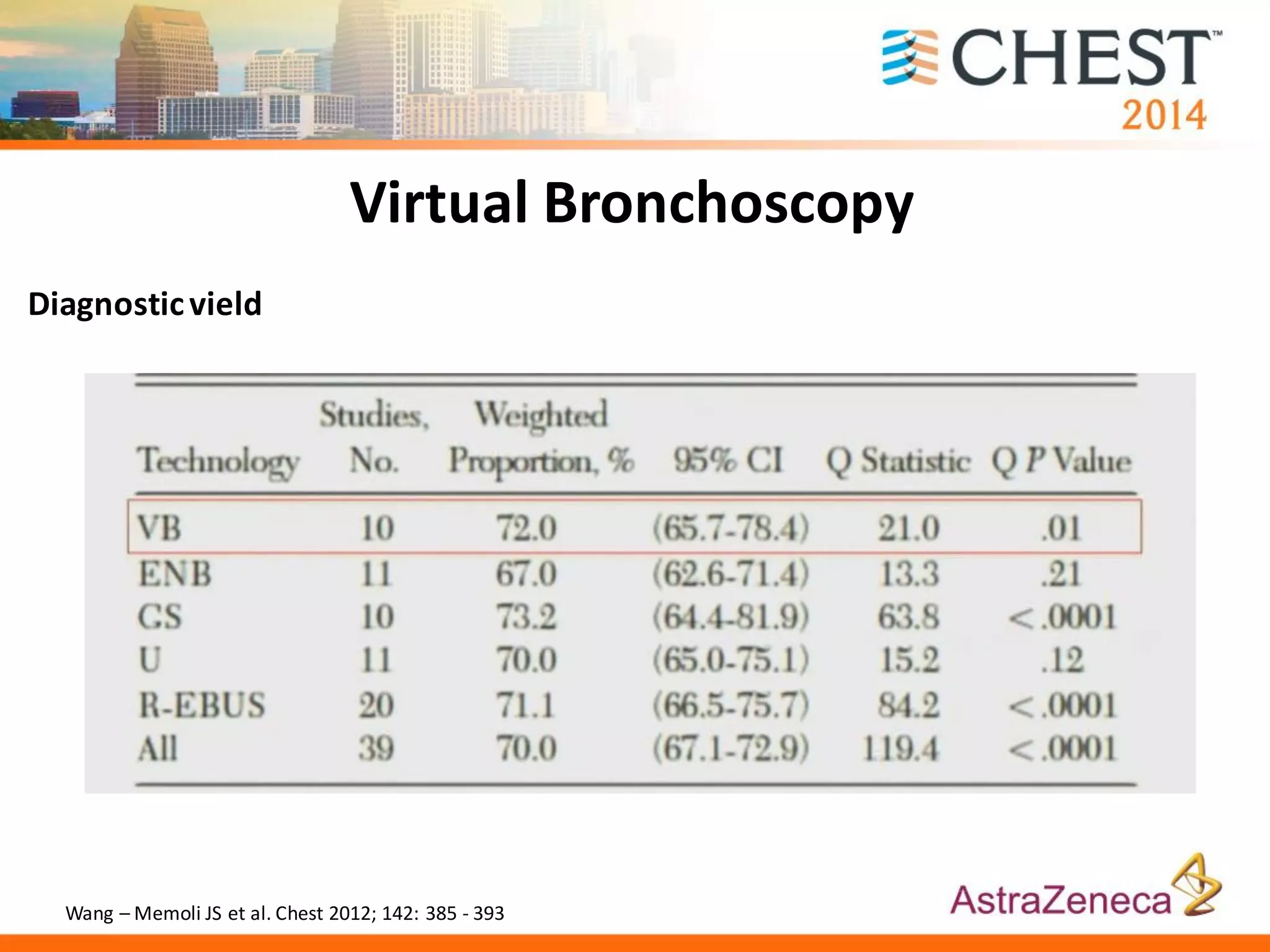
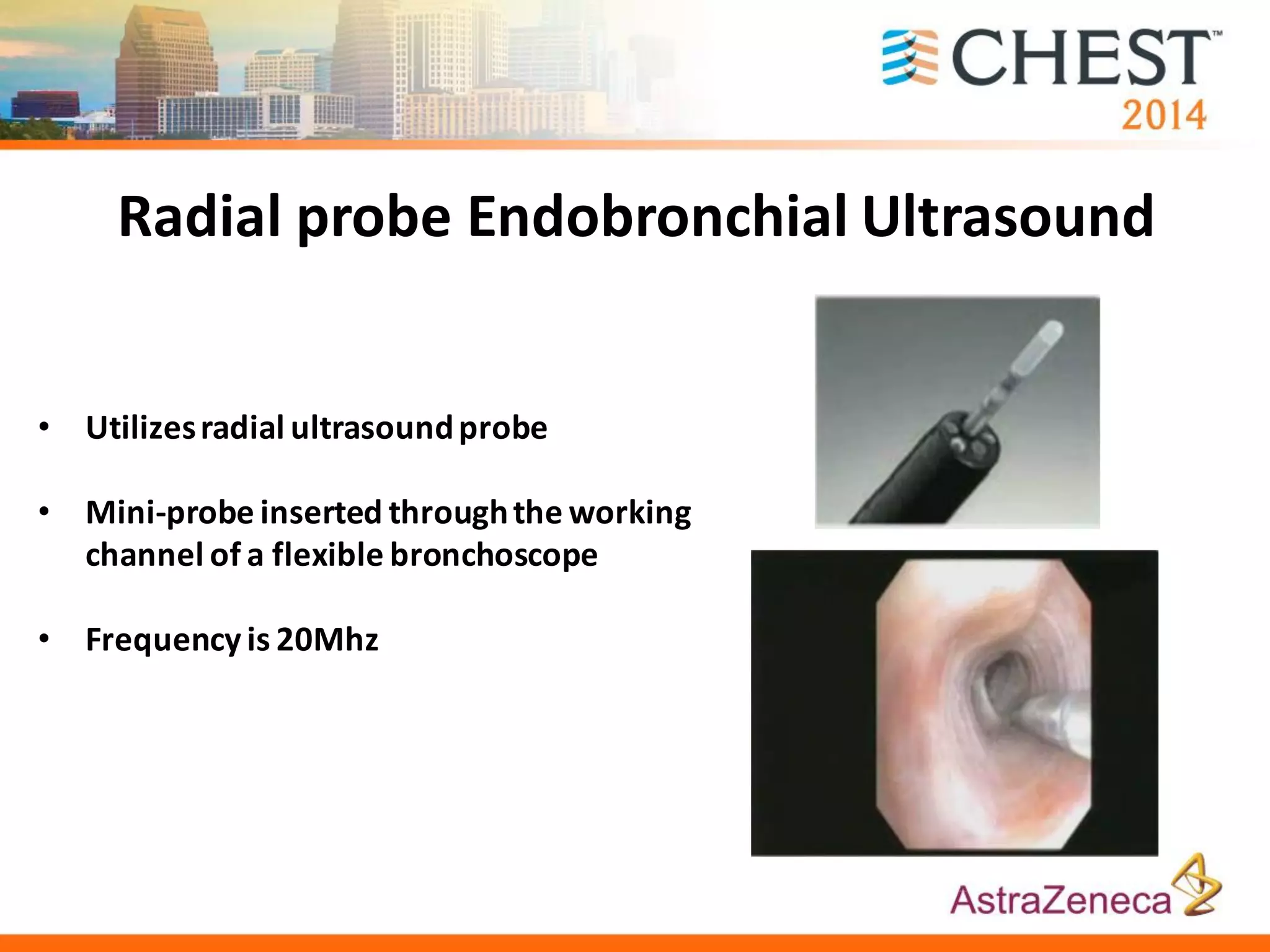
Comparison of diagnostic tools and techniques including radial EBUS, CT-guided aspiration, and virtual bronchoscopy.
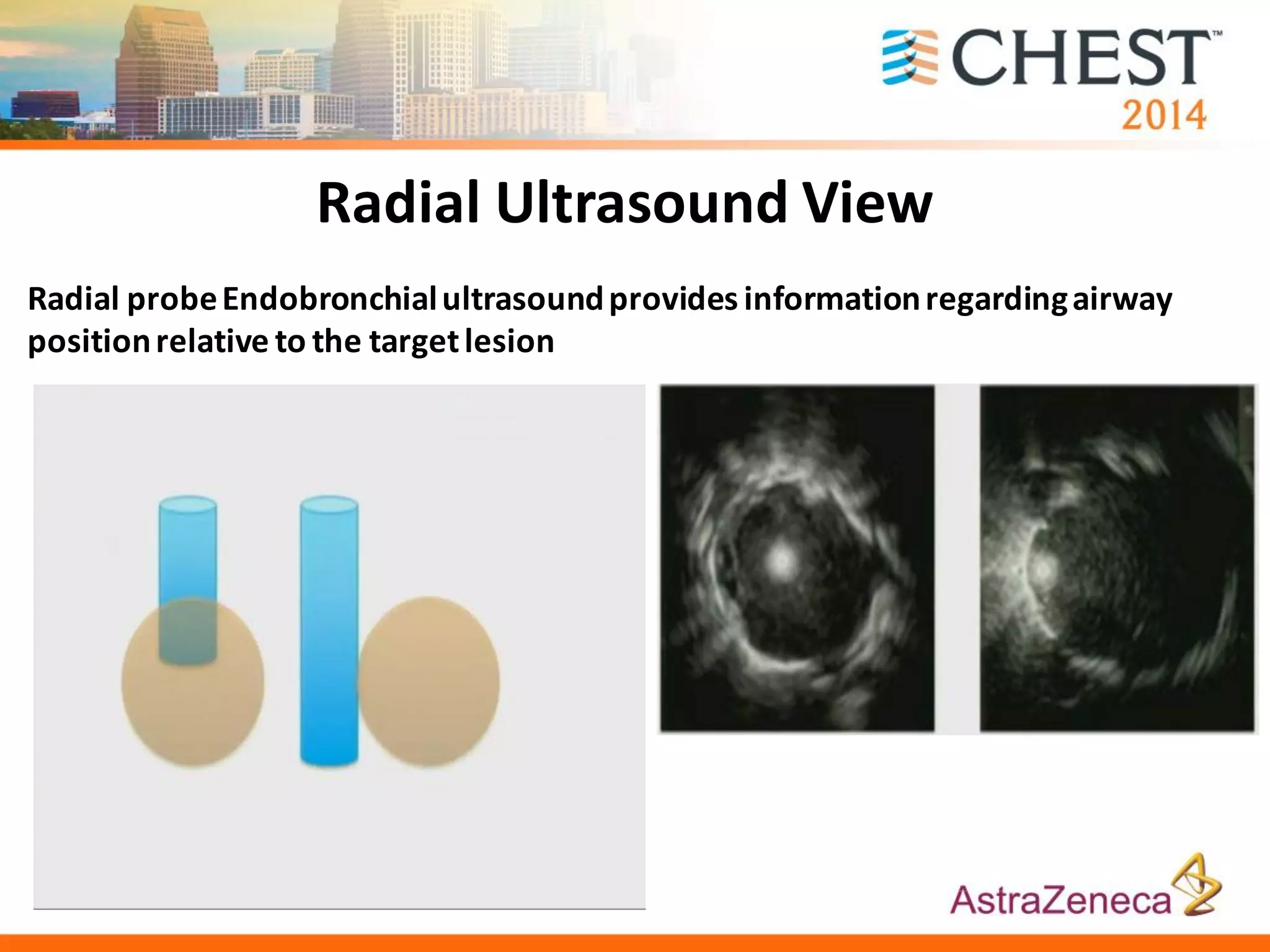
Enhanced utility of advanced diagnostic procedures using electromagnetic navigation and radial probe ultrasound in lung cancer.