The document discusses several topics:
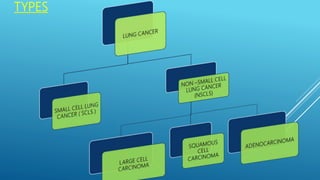
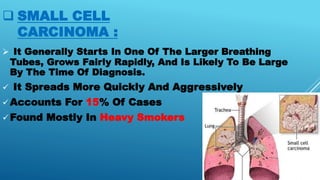
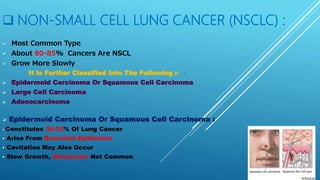
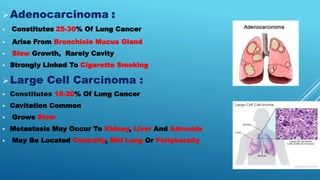
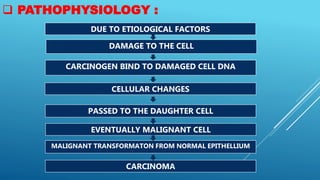
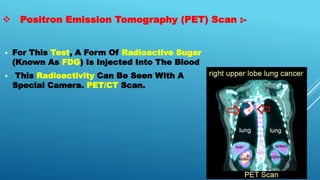
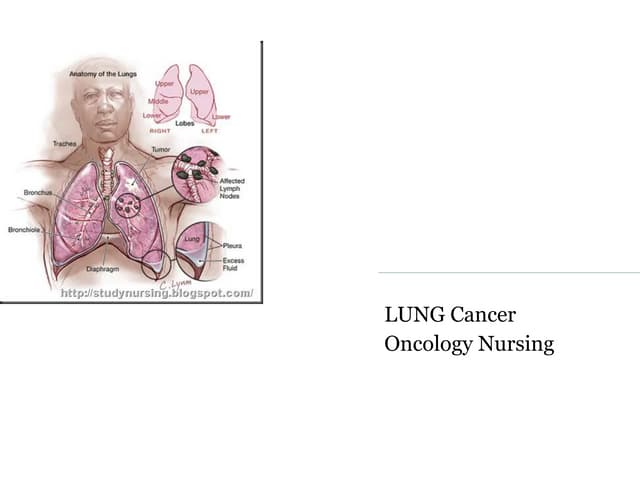
1. Lung cancer - it defines lung cancer, discusses types (small cell carcinoma and non-small cell carcinoma), staging, risk factors like smoking, signs and symptoms, diagnostic tests, and treatments.
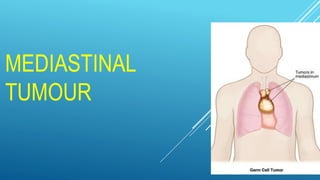
2. Mediastinal tumors - these are tumors located in the mediastinum, which can be malignant or benign. Signs and symptoms depend on location and compression of structures. Diagnosis involves imaging tests. Treatment includes radiation, chemotherapy, or surgery.
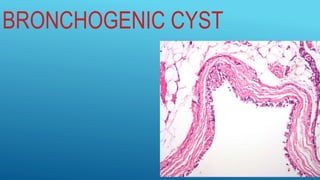
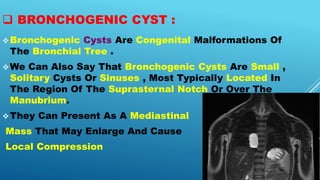
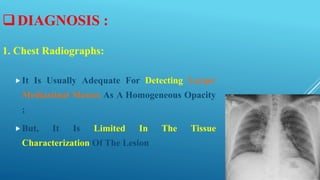
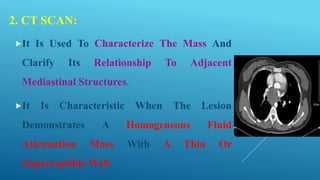
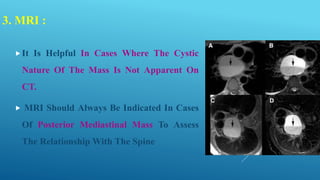
3. Bronchogenic cyst - this is a congenital malformation of the bronchial tree that presents as a mediastinal mass. It contains fluid and can enlarge, causing compression. Diagnosis involves imaging tests