Downloaded 12 times












































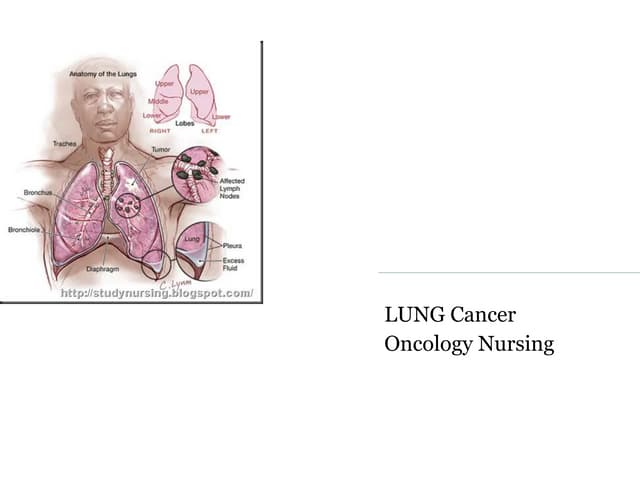
Lung cancer rates have improved only slightly over the past 50 years, with only 7% of cases cured in 1971 rising to 15% cured today. Lung cancer is classified as either small cell lung cancer, which is very aggressive, or non-small cell lung cancer, which includes squamous cell carcinoma, adenocarcinoma, and large cell carcinomas. The greatest risk factor is smoking tobacco, while other risks include radon exposure, lung diseases, and occupational hazards. Symptoms can include cough, breathing problems, weight loss, and chest pain, though early cancers may be asymptomatic. Diagnosis involves tests such as x-rays, CT scans, and biopsies. Treatment options include surgery, radiation, chemotherapy