Download as PDF, PPTX


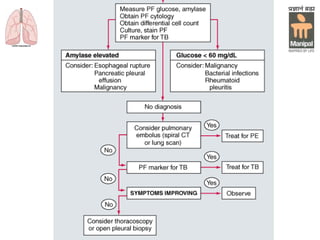

This document provides information on pleural diseases from the Department of Pulmonary Medicine. It discusses the anatomy and physiology of the pleura, and then summarizes different pleural conditions including pneumothorax, pleural effusion, and empyema. For each condition, it outlines the epidemiology, etiology, clinical features, investigations, and treatment. The document uses headings to separate each section and provides detailed information on evaluating and managing common pleural diseases.











































































































