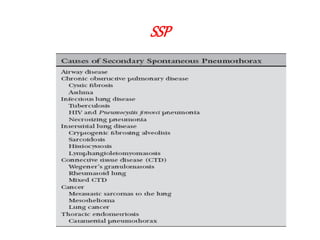
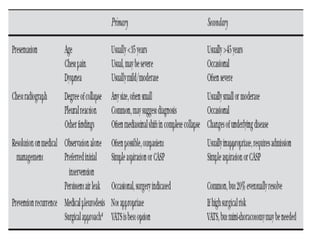
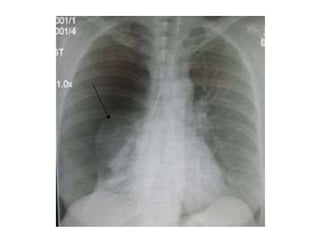
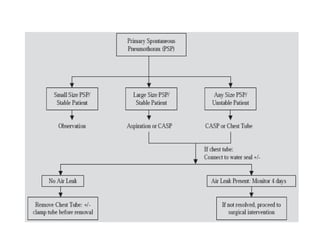
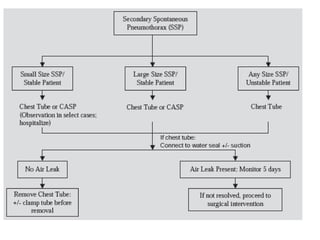
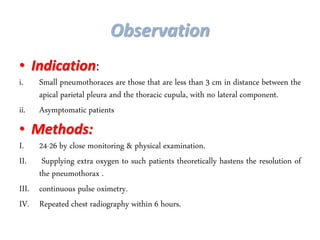
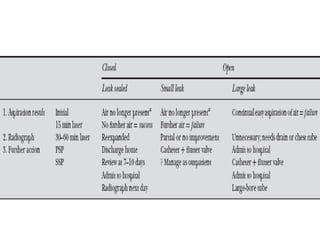
Pneumothorax is the presence of air in the pleural space, causing partial or complete lung collapse. It can be spontaneous or acquired through trauma or medical procedures. Spontaneous pneumothorax is often caused by subpleural bleb rupture in young, thin smokers and is classified as primary or secondary depending on underlying lung disease. Treatment depends on size and includes observation, needle aspiration, chest tube placement, chemical pleurodesis, or surgery like VATS for recurrent or large pneumothoraces. VATS allows inspection and bleb resection with pleurodesis to prevent recurrence in over 90% of patients.