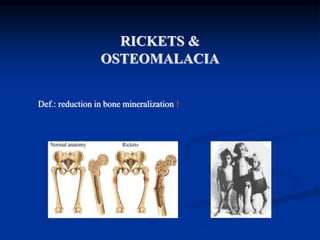
Rickets and osteomalacia are conditions caused by inadequate bone mineralization due to vitamin D deficiency. Rickets occurs in children and osteomalacia in adults. Vitamin D deficiency leads to decreased calcium absorption and secondary hyperparathyroidism, resulting in inadequate bone mineralization. People with these conditions experience bone pain and fractures. Diagnosis involves blood tests showing low calcium, phosphate and high alkaline phosphatase levels. Treatment involves high dose vitamin D and calcium supplementation.
INTRODUCTION — Normal bone growth and mineralization require adequate calcium and phosphate, the two major constituents of the crystalline component of bone. Deficient mineralization can result in rickets and/or osteomalacia. Rickets refers to deficient mineralization at the growth plate, as well as architectural disruption of this structure. Osteomalacia refers to impaired mineralization of the bone matrix. Rickets and osteomalacia usually occur together as long as the growth plates are open; only osteomalacia occurs after the growth plates have fused.
rickets is a nutritional deficiency disease that involves mainly calcium, vitamin d, or phosphate resulting in decreased bone stability and strength, Delayed closure of the fontanelles,Parietal and frontal bossing. Craniotabes (soft skull bones).
Enlargement of the costochondral junction visible as beading along the anterolateral aspects of the chest (the "rachitic rosary") . Formation of Harrison sulcus (or groove),Widening of the wrist and bowing of the distal radius and ulna, Progressive lateral bowing of the femur and tibia and causes defects in teeth.
there is two types of rickets: phosphopenic and calcipenic.
pathogenesis: Growth plate thickness is determined by two opposing processes: o chondrocyte proliferation and hypertrophy on the one hand. o vascular invasion of the growth plate followed by conversion into primary bone spongiosa on the other. • Vascular invasion requires mineralization of the growth plate cartilage and is delayed or prevented by deficiency of calcium or phosphorus growth plate cartilage accumulates and the growth plate thickens. • In addition, the chondrocytes of the growth plate become disorganized, losing their columnar orientation with characteristic expansion of the hypertrophic zone. • In the bone tissue below the growth plate (metaphysis), the mineralization defect leads to the accumulation of osteoid.
Osteomalacia is the softening of the bones caused by defective bone mineralization secondary to inadequate levels of available phosphate and calcium.
The true prevalence of osteomalacia across the globe remains unknown.
INTRODUCTION — Normal bone growth and mineralization require adequate calcium and phosphate, the two major constituents of the crystalline component of bone. Deficient mineralization can result in rickets and/or osteomalacia. Rickets refers to deficient mineralization at the growth plate, as well as architectural disruption of this structure. Osteomalacia refers to impaired mineralization of the bone matrix. Rickets and osteomalacia usually occur together as long as the growth plates are open; only osteomalacia occurs after the growth plates have fused.
rickets is a nutritional deficiency disease that involves mainly calcium, vitamin d, or phosphate resulting in decreased bone stability and strength, Delayed closure of the fontanelles,Parietal and frontal bossing. Craniotabes (soft skull bones).
Enlargement of the costochondral junction visible as beading along the anterolateral aspects of the chest (the "rachitic rosary") . Formation of Harrison sulcus (or groove),Widening of the wrist and bowing of the distal radius and ulna, Progressive lateral bowing of the femur and tibia and causes defects in teeth.
there is two types of rickets: phosphopenic and calcipenic.
pathogenesis: Growth plate thickness is determined by two opposing processes: o chondrocyte proliferation and hypertrophy on the one hand. o vascular invasion of the growth plate followed by conversion into primary bone spongiosa on the other. • Vascular invasion requires mineralization of the growth plate cartilage and is delayed or prevented by deficiency of calcium or phosphorus growth plate cartilage accumulates and the growth plate thickens. • In addition, the chondrocytes of the growth plate become disorganized, losing their columnar orientation with characteristic expansion of the hypertrophic zone. • In the bone tissue below the growth plate (metaphysis), the mineralization defect leads to the accumulation of osteoid.
Osteomalacia is the softening of the bones caused by defective bone mineralization secondary to inadequate levels of available phosphate and calcium.
The true prevalence of osteomalacia across the globe remains unknown.
Calcium metabolism disorders
1. CALCIUM METABOLISM DISORDERS
2. OVERVIEW: Calcium definition and requirement . Calcium metabolism regulators : VD , PTH and calcitonin. Functions of calcium. Calcium metabolic bone diseases. Calcium metabolism disorders. CASE !!
3. WHAT IS CALCIUM? Calcium is a mineral that is essential to bone health, cardiovascular health, muscle maintenance, circulatory health, and blood clotting. Calcium also acts as an enzyme activator. While calcium is found in milk and dairy products, it is also available from other food sources, such as green leafy vegetables, seafood (eating salmon with the bones provides an even greater dose), almonds, blackstrap molasses, broccoli, enriched soy and rice milk products, figs, soybeans and tofu.
Macroeconomics- Movie Location
This will be used as part of your Personal Professional Portfolio once graded.
Objective:
Prepare a presentation or a paper using research, basic comparative analysis, data organization and application of economic information. You will make an informed assessment of an economic climate outside of the United States to accomplish an entertainment industry objective.
Acetabularia Information For Class 9 .docxvaibhavrinwa19
Acetabularia acetabulum is a single-celled green alga that in its vegetative state is morphologically differentiated into a basal rhizoid and an axially elongated stalk, which bears whorls of branching hairs. The single diploid nucleus resides in the rhizoid.
Embracing GenAI - A Strategic ImperativePeter Windle
Artificial Intelligence (AI) technologies such as Generative AI, Image Generators and Large Language Models have had a dramatic impact on teaching, learning and assessment over the past 18 months. The most immediate threat AI posed was to Academic Integrity with Higher Education Institutes (HEIs) focusing their efforts on combating the use of GenAI in assessment. Guidelines were developed for staff and students, policies put in place too. Innovative educators have forged paths in the use of Generative AI for teaching, learning and assessments leading to pockets of transformation springing up across HEIs, often with little or no top-down guidance, support or direction.
This Gasta posits a strategic approach to integrating AI into HEIs to prepare staff, students and the curriculum for an evolving world and workplace. We will highlight the advantages of working with these technologies beyond the realm of teaching, learning and assessment by considering prompt engineering skills, industry impact, curriculum changes, and the need for staff upskilling. In contrast, not engaging strategically with Generative AI poses risks, including falling behind peers, missed opportunities and failing to ensure our graduates remain employable. The rapid evolution of AI technologies necessitates a proactive and strategic approach if we are to remain relevant.
Biological screening of herbal drugs: Introduction and Need for
Phyto-Pharmacological Screening, New Strategies for evaluating
Natural Products, In vitro evaluation techniques for Antioxidants, Antimicrobial and Anticancer drugs. In vivo evaluation techniques
for Anti-inflammatory, Antiulcer, Anticancer, Wound healing, Antidiabetic, Hepatoprotective, Cardio protective, Diuretics and
Antifertility, Toxicity studies as per OECD guidelines
Francesca Gottschalk - How can education support child empowerment.pptxEduSkills OECD
Francesca Gottschalk from the OECD’s Centre for Educational Research and Innovation presents at the Ask an Expert Webinar: How can education support child empowerment?
The Roman Empire A Historical Colossus.pdfkaushalkr1407
The Roman Empire, a vast and enduring power, stands as one of history's most remarkable civilizations, leaving an indelible imprint on the world. It emerged from the Roman Republic, transitioning into an imperial powerhouse under the leadership of Augustus Caesar in 27 BCE. This transformation marked the beginning of an era defined by unprecedented territorial expansion, architectural marvels, and profound cultural influence.
The empire's roots lie in the city of Rome, founded, according to legend, by Romulus in 753 BCE. Over centuries, Rome evolved from a small settlement to a formidable republic, characterized by a complex political system with elected officials and checks on power. However, internal strife, class conflicts, and military ambitions paved the way for the end of the Republic. Julius Caesar’s dictatorship and subsequent assassination in 44 BCE created a power vacuum, leading to a civil war. Octavian, later Augustus, emerged victorious, heralding the Roman Empire’s birth.
Under Augustus, the empire experienced the Pax Romana, a 200-year period of relative peace and stability. Augustus reformed the military, established efficient administrative systems, and initiated grand construction projects. The empire's borders expanded, encompassing territories from Britain to Egypt and from Spain to the Euphrates. Roman legions, renowned for their discipline and engineering prowess, secured and maintained these vast territories, building roads, fortifications, and cities that facilitated control and integration.
The Roman Empire’s society was hierarchical, with a rigid class system. At the top were the patricians, wealthy elites who held significant political power. Below them were the plebeians, free citizens with limited political influence, and the vast numbers of slaves who formed the backbone of the economy. The family unit was central, governed by the paterfamilias, the male head who held absolute authority.
Culturally, the Romans were eclectic, absorbing and adapting elements from the civilizations they encountered, particularly the Greeks. Roman art, literature, and philosophy reflected this synthesis, creating a rich cultural tapestry. Latin, the Roman language, became the lingua franca of the Western world, influencing numerous modern languages.
Roman architecture and engineering achievements were monumental. They perfected the arch, vault, and dome, constructing enduring structures like the Colosseum, Pantheon, and aqueducts. These engineering marvels not only showcased Roman ingenuity but also served practical purposes, from public entertainment to water supply.
June 3, 2024 Anti-Semitism Letter Sent to MIT President Kornbluth and MIT Cor...Levi Shapiro
Letter from the Congress of the United States regarding Anti-Semitism sent June 3rd to MIT President Sally Kornbluth, MIT Corp Chair, Mark Gorenberg
Dear Dr. Kornbluth and Mr. Gorenberg,
The US House of Representatives is deeply concerned by ongoing and pervasive acts of antisemitic
harassment and intimidation at the Massachusetts Institute of Technology (MIT). Failing to act decisively to ensure a safe learning environment for all students would be a grave dereliction of your responsibilities as President of MIT and Chair of the MIT Corporation.
This Congress will not stand idly by and allow an environment hostile to Jewish students to persist. The House believes that your institution is in violation of Title VI of the Civil Rights Act, and the inability or
unwillingness to rectify this violation through action requires accountability.
Postsecondary education is a unique opportunity for students to learn and have their ideas and beliefs challenged. However, universities receiving hundreds of millions of federal funds annually have denied
students that opportunity and have been hijacked to become venues for the promotion of terrorism, antisemitic harassment and intimidation, unlawful encampments, and in some cases, assaults and riots.
The House of Representatives will not countenance the use of federal funds to indoctrinate students into hateful, antisemitic, anti-American supporters of terrorism. Investigations into campus antisemitism by the Committee on Education and the Workforce and the Committee on Ways and Means have been expanded into a Congress-wide probe across all relevant jurisdictions to address this national crisis. The undersigned Committees will conduct oversight into the use of federal funds at MIT and its learning environment under authorities granted to each Committee.
• The Committee on Education and the Workforce has been investigating your institution since December 7, 2023. The Committee has broad jurisdiction over postsecondary education, including its compliance with Title VI of the Civil Rights Act, campus safety concerns over disruptions to the learning environment, and the awarding of federal student aid under the Higher Education Act.
• The Committee on Oversight and Accountability is investigating the sources of funding and other support flowing to groups espousing pro-Hamas propaganda and engaged in antisemitic harassment and intimidation of students. The Committee on Oversight and Accountability is the principal oversight committee of the US House of Representatives and has broad authority to investigate “any matter” at “any time” under House Rule X.
• The Committee on Ways and Means has been investigating several universities since November 15, 2023, when the Committee held a hearing entitled From Ivory Towers to Dark Corners: Investigating the Nexus Between Antisemitism, Tax-Exempt Universities, and Terror Financing. The Committee followed the hearing with letters to those institutions on January 10, 202
3. Vitamin D Deficiency
Osteomalacia & Rickets
Osteomalacia occurs in adults
Rickets occurs in children
Defective mineralization of the skeleton
4. VITAMIN D DEFICIENCY
Vitamin D deficiency leads to decreased absorptio
n of calcium by the GI tract.
As serum calcium starts to fall, secondary hyperpar
athyroidism occurs.
5. VITAMIN D DEFICIENCY
Elevated Pth levels may maintain serum calcium in
the normal range, but at the cost of phosphaturia,
hypophosphatemia and increased bone reabsorptio
n
Low serum phosphate results in inadequate bone
mineralization and osteopenia.
6. VITAMIN D DEFICIENCY
In severe cases, secondary hyperparathyroidism is
not adequate to maintain serum calcium levels, an
d hypocalcemia occurs.
7. OSTEOMALACIA,RICKETS
Regulation of Calcium & Phosphate Metabolism:
Peak bone mass at 16-25 years.
Bone loss 0.3- 0.5% per year (2-3% per year after 6th decade).
1. Parathyroid Hormone (PTH)
2. Vitamin D3
3. Calcitonin
4. Other Hormones: Est
rogen: Prevents bone loss
Corticosteroids: Increases bone loss
Thyroid hormones: Leads to osteoporosis
Growth hormones: Cause positive calcium balance
Growth factors
8. Biochemistry of Vitamin D3 – Bri
ef Review
Vitamin D3 (cholecalciferol) is synthesize
d in the skin, with UV light, from 7-dehy
drocholesterol
Vitamin D3 is hydroxylated twice – first i
n the liver, to 25-hydroxycholecalciferol, t
hen in the kidney, to 1, 25-dihydroxychol
ecalciferol, the most potent form of Vita
min D
9. Vitamin D (cont’)
Primary role of Vitamin D
Increase calcium and phosphate absorption from the
intestines
Other tissues that Vitamin D acts on
Parathyroid glands
Bone, Kidneys
Skin, Brain, Pituitary
Lymphocytes,Tumors
10. Other conditions that can cause Oste
omalacia
Hereditary or acquired disorders of vitamin D meta
bolism
Kidney failure and acidosis
Phosphate depletion associated with not enough ph
osphates in the diet
Cancer
Side effects of medications used to treat seizures (D
ilantin)
Liver disease
11. RICKETS, OSTEOMALACIA
PATHOLOGY:
Sufficient osteoid, poor mineralization
(Rickets is found only in children prior to the closure of the growt
h plates, while OSTEOMALACIA occurs in persons of any ag
e. Any child with rickets also has osteomalacia, while the rever
se is not necessarily true).
12. RICKETS, OSTEOMALACIA
CAUSES:
1. Nutritional deficiency
1. Vit D
2. chelators of calcium- phytates, oxalates, phosphorous
3. Antacid abuse, causing reduced dietary phosphate binding
2. GI Absorption defects
1. Post gastrectomy
2. Biliary disease (reduced absorption of Vitamins )
3. Small bowel disease
4. liver disease
3. Renal tubular defects
4. Renal osteodystrophy
5. Miscellaneous causes
13. Vitamin D Deficiency
Osteomalacia & Rickets (cont’)
Secondary to many things, including
Vitamin D deficiency as discussed above
Dietary calcium deficiency
Phosphorus deficiency
Aluminum toxicity
Hypophosphatasia
Fibrogenesis imperfecta ossium
14. Clinical features
Osteomalacia in adults starts insidiously as aches and pains in the lu
mbar (lower back) region and thighs, spreading later to the arms and
ribs.
Pain is non-radiating, symmetrical, and accompanied by tenderness i
n the involved bones.
Proximal muscles are weak, and there is difficulty in climbing up sta
irs and getting up from a squatting position.
Physical signs include deformities like and lordosis.
Pathologic fractures due to weight bearing may develop.
Most of the time, the only alleged symptom is chronic and bone ach
es are not spontaneous but only revealed by pressure or shocks.
15. RICKETS, OSTEOMALACIA
CLINICAL FEATURES:
Rickets - Tet
any , convulsions, failure to thrive, restles
sness, muscular flaccidity. Flattening of
skull (craniotabes), Thickening of wris
ts from epiphyseal overgrowth, Stunted growth,
Rickety rosary, spinal curvature, C
oxa vara, bowing, # of long bones
Osteomalacia, - Aches and pains, muscle weakness loss of hei
ght, stress #s.
16. Manifestations of Osteomalacia
Localized bone pain
Difficulty walking
Low back pain
Fractures are common, and delayed healing occu
rs
Muscular weakness
Weight loss
Progressive deformities of the spine (kyphosis)
17. Rickets, clinical manifestations
Skeletal findings:
1. Delay in closure of the fontanelles.
2. Parietal & frontal bossing.
3. Craniotabes ( soft skull bones).
4. Enlargement of the costochondral junction (rachitic rosary).
5. The development of Harrison sulcus ( caused by pull of the diaphragmatic attachments
to the lower ribs).
6. Enlargement of the wrist & bowing of the distal radius & ulna.
7. Progressive lateral bowing of the femur & tibia.
19. RICKETS, OSTEOMALACIA
XRAY FINDINGS:
OSTEOMALACIA
Loosers zones - incomplete str
ess # with healing lacking ca
lcium, on compression side
of long bones.
Codfish vertebrae due to press
ure of discs
Trefoil pelvis, due to indentatio
n of acetabulae stress #s
20.
21. Osteomalacia & Rickets – Clinica
l Manifestations
Asymptomatic at onset
Muscle weakness, especially of pe
lvic girdle
Bone pain
Atraumatic fractures
X-rays assist in diagnosis
22. RICKETS, OSTEOMALACIA
INVESTIGATIONS:
BLOOD TESTS Calci
um Reduced, Phosphate r
educed Alkalline Phosph
atase increased Urinary excretion of c
alcium diminished
Calcium phosphate products (= serum [Ca] x serum [PO4]) norm
ally 30. In rickets and osteomalacia is less than 24
23. Osteomalacia & Rickets - Diagno
sis
Other laboratory abnormalities may include
Hypocalcemia
Hypophosphatemia
Elevated serum alkaline phosphatase
24. Biochemical findings in rickets
Alkaline phosphatase usually is ↑in all forms of rickets.
Serum phosphorus concentrations usually are↓ in both hypocalcemic and hyp
ophosphatemic rickets.
Serum Ca is ↓only in hypocalcemic rickets.
Serum parathyroid hormone typically is ↑in hypocalcemic rickets, in contrast i
t is N in hypophosphatemic rickets.
25-OH vitamin D reflect the amount of vitamin D stored in the body, and is
↓in vit D deficiency.
1,25-OH2 vitamin D can be↓, N or ↑in hypocalcemic rickets and usually is N
or slightly ↑in hypophosphatemic rickets.
25. Osteomalacia & Rickets - Diagno
sis
Bone biopsy is diagnostic
Serum 25-hydroxycholecalciferol <50nmol/L in
dicates Vitamin D deficiency
26. OSTEOMALACIA:
EVALUATION
Careful diet and sunlight history
Renal function
Fecal fat determination
Anti IgA tissue transglutaminase antibodies.
Small bowel biopsy
27. RICKETS, OSTEOMALACIA
MANAGEMENT:
Depends on the cause
Nutritional Vitami
n D deficiency Dietary che
lators of calcium
Phytates
Oxalates Phospho
rus deficiency (unusual)
Antacid abuse
Treatment- vitamin D (50000u/w`/up to 3-12 w) and Calciu
m (1.5-2g/day)
28. RICKETS, OSTEOMALACIA
MANAGEMENT:
Depends on the cause
Gastro-intestinal absorption defects Po
st-gastrectomy Biliary
disease Enteric abs
orption defects
Short bowel syndrome
Rapid onset (gluten-sensitive enteropathy) Inflamm
atory bowel disease
Crohns
Celiac
29. RICKETS, OSTEOMALACIA
MANAGEMENT:
Depends on the cause
Renal tubular defects Vita
min D dependant
type I
type II
Treatment; High levels of vit D
Vitam
in D resistant (familial hypophosphatemic rickets)
Treatment; Phosphate 1-3 gm daily, Vit D3 high dose
Fanconi syndrome I, II, III R
enal tubular acidosis
30. Vitamin D Deficiency - Treatmen
t
50,000 IU of oral Vitamin D2, once or twic
e weekly for 6 – 12 w, followed by 1000 IU
/day
Appropriate exposure to sunlight
Phosphate and Calcium replacement, if nee
ded
Editor's Notes
Diffuse (not pinpointed to one location) bone pain, especially in the hips
Muscle weakness
Bone fractures that happen with very little trauma
Symptoms associated with low calcium including:
Numbness around the mouth
Numbness of extremities
Spasms of hands or feet
Abnormal heart rhythms