Downloaded 64 times

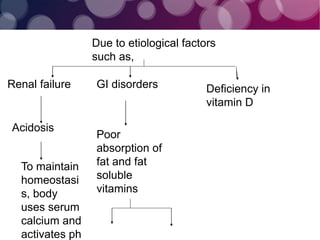
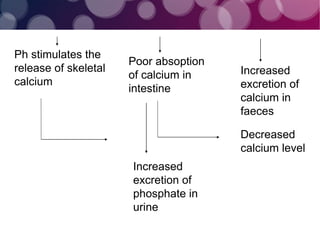


Osteomalacia, also known as adult rickets, is a metabolic bone disease characterized by inadequate mineralization caused by vitamin D deficiency, leading to softening of bones, pain, and fractures. Key factors contributing to the disease include poor diet, lack of sunlight, and various medical conditions affecting calcium and phosphate metabolism. Management involves dietary modifications, vitamin D supplementation, and potentially surgical interventions for orthopedic deformities.




























![Osteomalacia 2nd-150704155942-lva1-app6892 [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/osteomalacia-2nd-150704155942-lva1-app6892autosaved-200520081743-thumbnail.jpg?width=640&height=640&fit=bounds)





















![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)















