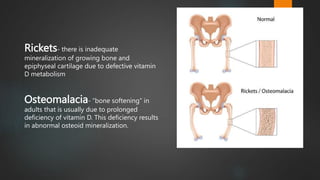
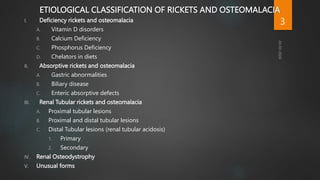
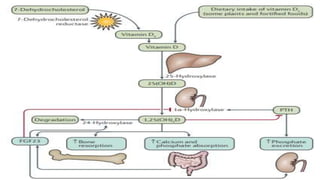
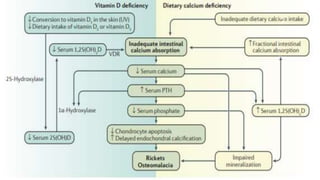
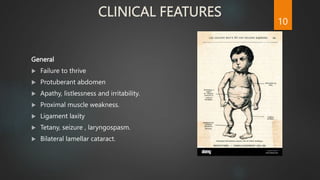
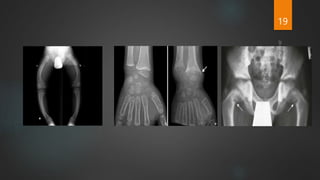
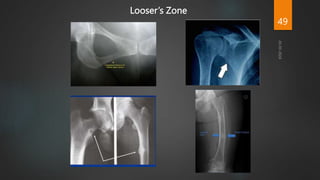
Rickets and osteomalacia are caused by defective vitamin D metabolism and mineralization of bone. Rickets occurs in children and results in inadequate bone mineralization and deformities, while osteomalacia is a softening of bones in adults. Causes include vitamin D deficiency, disorders of calcium or phosphate absorption, and certain medical conditions like renal tubular disorders. Symptoms vary depending on location but include bone pain, weakness, and deformities. Treatment involves addressing the underlying cause, usually with vitamin D and mineral supplementation. Ongoing monitoring is needed to ensure healing and prevent long-term complications.
















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















