Downloaded 53 times
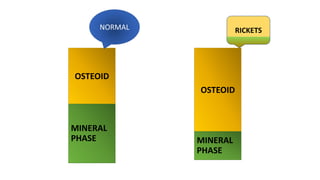












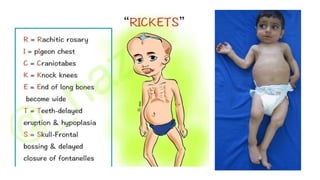



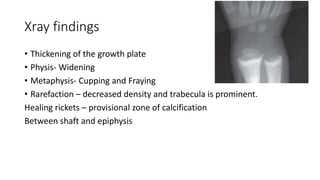














Rickets is a disease of growing bone caused by unmineralized bone matrix at the growth plates, occurring only in children before fusion of the epiphyses. It is caused by vitamin D disorders, calcium deficiency, renal losses, or phosphorous deficiency. Clinical features include failure to thrive, bowed legs, widened wrists and ankles, and bone pain. X-rays show widened growth plates and fraying and cupping of the metaphysis. Treatment involves high dose vitamin D and calcium supplementation.























































































