This document discusses orbital cellulitis and its causes, signs, symptoms, investigations, differential diagnosis, treatment and complications. Some key points:
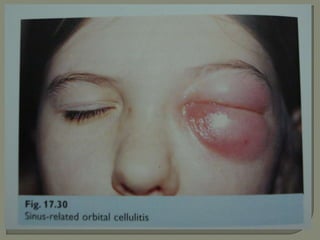
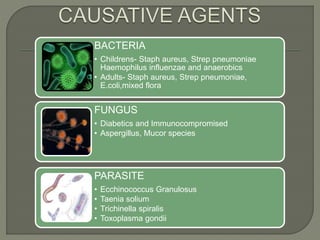
- Orbital cellulitis is an infection of the soft tissues of the eyelids and orbit. It is usually caused by Staphylococcus aureus or Streptococcus bacteria spreading from nearby infections.
- Symptoms include eyelid swelling, pain, redness and fever. Proptosis and vision issues may occur if the infection spreads to the orbit.
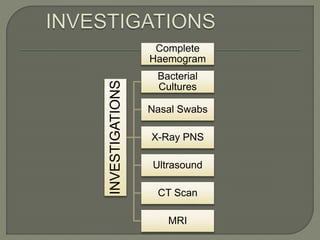
- Diagnosis involves examination, blood tests and imaging like CT scans. Broad-spectrum antibiotics are the primary treatment. Surgery may be needed to drain abscesses. Complications can include vision loss, ca
























































![Lenstar ls 900[1]](https://cdn.slidesharecdn.com/ss_thumbnails/lenstarls9001-120626090045-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)














































































