Downloaded 1,574 times
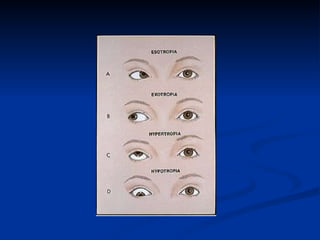
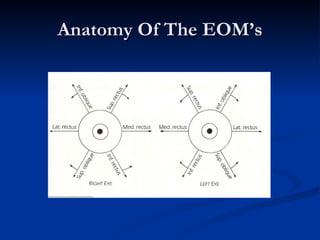
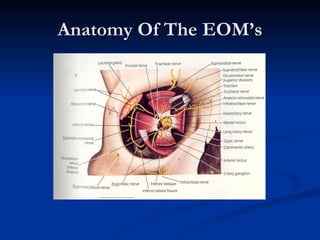
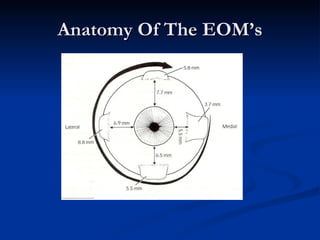
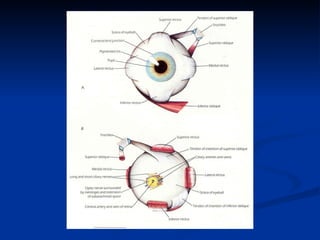
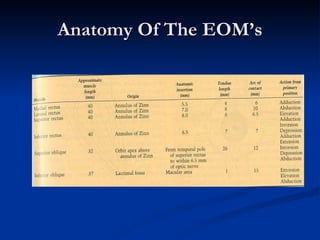




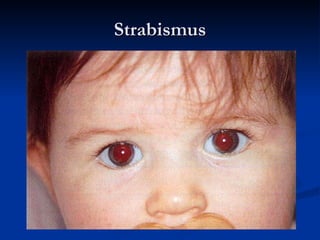

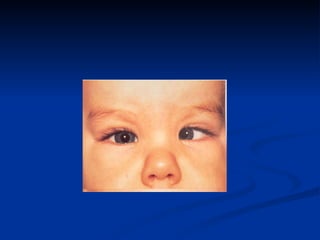
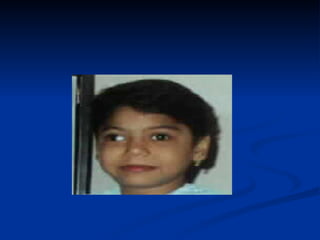


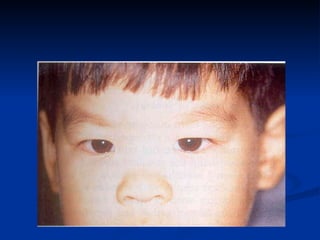
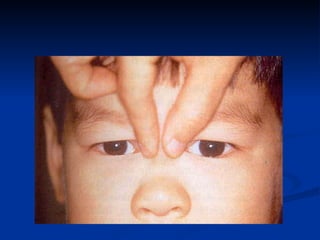
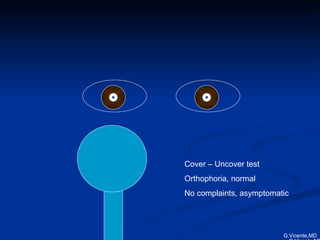
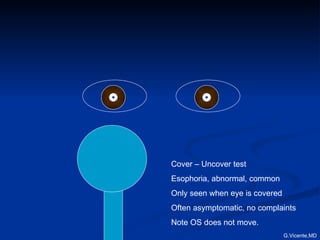
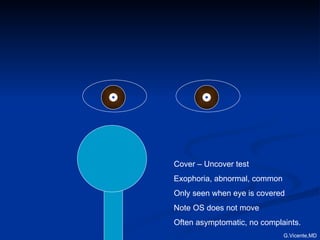
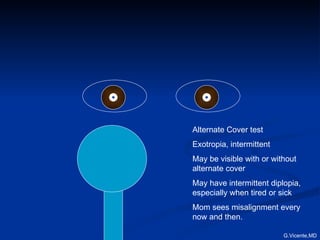
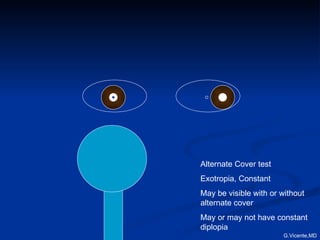
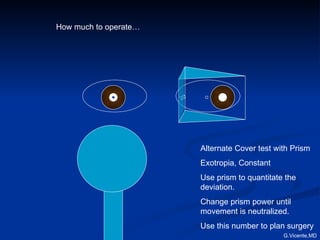


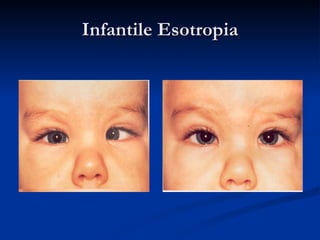
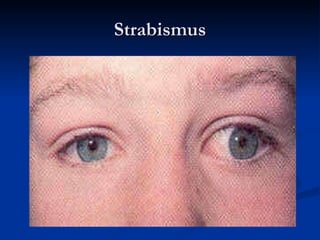


The document discusses strabismus, also known as squint or crossed eyes, covering its definition, anatomy, classification, types of amblyopia, and treatment options. Key components include the anatomy of the extraocular muscles, the reasons for treatment such as restoring stereopsis and preventing amblyopia, and detailed insights into various types of esotropia and exotropia. Management strategies are highlighted, including the importance of early intervention, surgical options, and the role of glasses in treatment.


















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















