This document discusses various types of cataracts, their causes, symptoms and management. It describes how cataracts can be primary/age-related or secondary due to other ocular diseases, systemic conditions like diabetes or medications. Trauma is also a common cause of unilateral cataract in young individuals. The document provides details on clinical findings, mechanisms and treatment of different cataract subtypes.

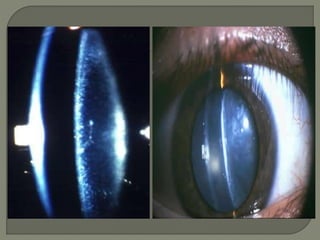


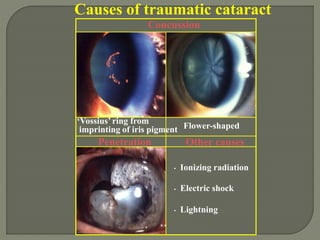
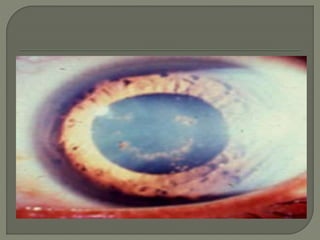
![ A ring-shaped anterior subcapsular opacity may underlie a
Vossius ring [ Imprinting of iris pigment on anterior lens
capsule]
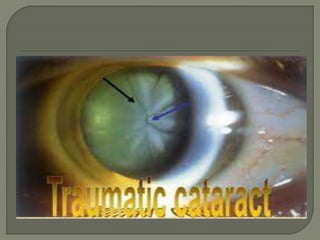
Commonly opacification occurs in the posterior subcapsular
cortex resulting in flower -shaped opacity [rossette] which
may subsequently disappear, remain stationary or progress to
maturity.
Cataract surgery may be necessary for visually significant
opacity.
Lens protein leak can lead to secondary Glaucoma,uveitis.](https://image.slidesharecdn.com/metaboliccomplicatedcataract-230611110126-dd393e81/85/Metabolic-complicated-cataract-pptx-37-320.jpg)