Downloaded 566 times
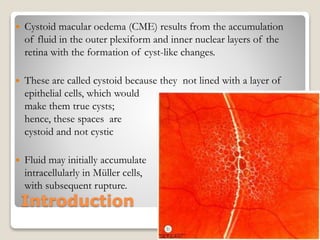

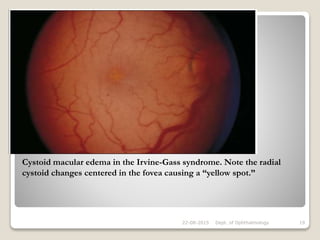






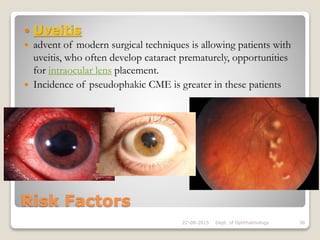













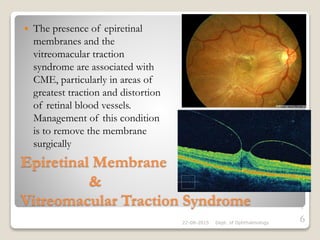
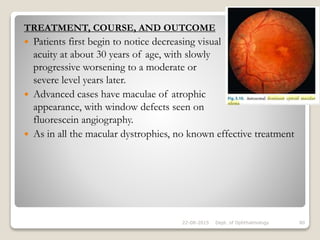


This document discusses cystoid macular edema (CME), including its pathogenesis, etiology, associated ocular conditions, manifestations, diagnosis and testing. Specifically, it focuses on pseudophakic or Irvine-Gass syndrome CME, which can occur after cataract surgery. The summary discusses how CME results from fluid accumulation in the retina, its appearance on fluorescein angiography, risk factors for pseudophakic CME like vitreous loss during surgery, and how it is diagnosed using techniques like optical coherence tomography.











































































