

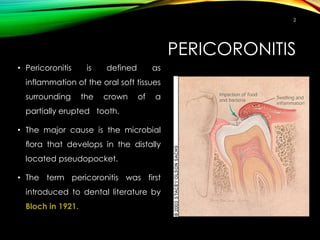
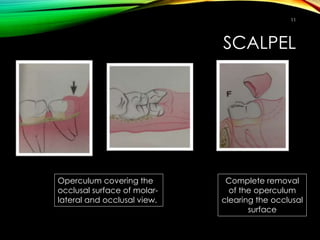


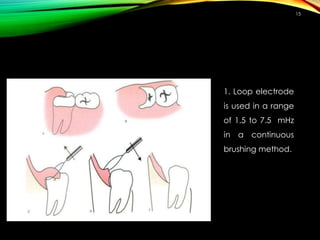

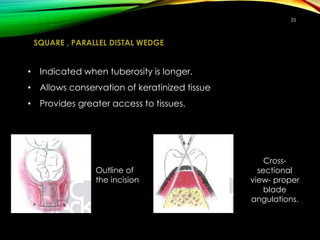
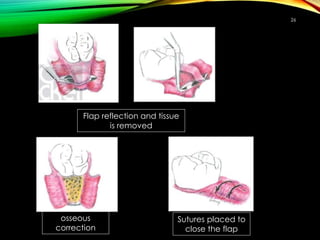


Pericoronitis is the inflammation of soft tissues around a partially erupted tooth, primarily caused by harmful microbial flora. Clinical features include pain, swelling, and potential complications like abscess formation, while treatment options include extraction and operculectomy using various techniques such as scalpel, electrocautery, and lasers. The document outlines the characteristics of acute, sub-acute, and chronic pericoronitis, along with tissue management during surgical procedures.

















































































