
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Oroantral Fistula
Similar to Oroantral Fistula (20)
Recently uploaded
Recently uploaded (20)
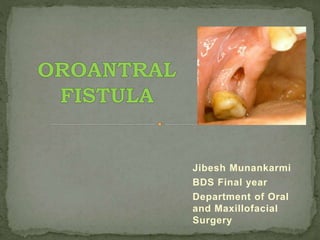
Oroantral Fistula
- 1. Jibesh Munankarmi BDS Final year Department of Oral and Maxillofacial Surgery
- 2. Introduction Definition Etiology Symptoms Diagnosis Management References
- 3. The maxillary sinus is the pneumatic space that is lodged inside the body of maxilla and that communicates with the environment by the way of middle nasal meatus and nasal vestibul -Orban`s
- 4. It is also known as Antrum of highmore. They are two in number, one on either side of the maxilla, and they are the largest of paranasal air sinuses. It can be described as pyramidal in shape, consisting of a base, an apex and four sides. Base: lateral wall of the nose Apex: projects laterally into zygomatic process of maxilla Four walls are formed by: 1. The roof of antrum or the floor of orbit 2. The anterior 3. Infratemporal surface of body of maxilla 4. The alveolar process of maxilla which is the floor of the sinus
- 5. • An oroantral perforation is an unnatural communication between the oral cavity and maxillary sinus. • An oroantral fistula is an epithelialized, pathological, unnatural communication between these two cavities.
- 6. • Extraction of teeth • Destruction of the portion of the floor of the sinus by periapical lesions • Perforation of the floor of the sinus and sinus membrane with injudicious use of instruments • Forcing a tooth or a root into the sinus during attempted removal • Extensive trauma to face • Chronic infection of maxillary sinus, such as osteomyelitis • Infected maxillary implant dentures • Malignancy involving the maxillary sinus such as malignant granuloma • Removal of a large cyst or resection of large tumour involving maxilla
- 7. IN FRESHOROANTRAL COMMUNICATION: 5 Es: 1. Escape of fluids: from mouth to the nose on the side of extraction. This happens when the patient rinses or gargles the mouth following the extraction of a tooth. 2. Epistaxis(unilateral): it is due to blood in the sinus escaping through osteum into the nostril. It may or may not be associated with frothing at nostril on the affected side. 3. Escape of air: from mouth into the nose, on sucking, inhaling or drawing on a cigarette, or puffing the cheeks.
- 8. 4. Enhanced column of air: causes alteration in vocal resonance and subsequently change in the voice. 5. Excruciating pain: in and around the region of the affected sinus, as the local anesthesia begins to wear off.
- 9. IN LATE STAGE, ESTABLISHED OROANTRAL FISTULA: 5 Ps: 1. Pain 2. Persistent, purulent or mucopurulent, foul, unilateral nasal discharge from the affected nostril, especially when head is lowered down. Unilateral foul or foetid taste and smell. 3. Postnasal drip: the trickling of the nasal discharge from the posterior nares, down the pharynx. The continuous swallowing of the foul mucopurulent discharge may lead to unpleasant taste. This is accompanied by nocturnal cough, hoarseness, ear ache or catarrhal deafness.
- 10. 4. Possible sequelae of general systemic toxemic condition: fever, malaise, morning anorexia, frontal and parietal headaches and in extreme cases anosmia and cacosmia. 5. Popping out of an antral polyp: the persistent infection in the antrum may lead to establishment of chronic long standing oroantral fistula, which may be occluded by an antral polyp. This can be seen as a bluish red lump extruding through the fistula.
- 11. PHYSICAL SIGNS OF ESTABLISHED OROANTRAL FISTULA: Early signs: The early signs are seen when the blood clot gets disintegrated, so that the breach in the continuity of antral lining remains patent; a) As a result of infection b) Forceful nose blowing c) Excessive rinsing of mouth Late signs and symptoms: Due to involvement of sinusitis or established oroantral fistula with or without rhinitis; a) Signs and symptoms of sinusitis and rhinits b) Escape of air or fluid through nostril c) Development a lump(polyp) On examination: •Discharge of foul smelling pus from the orifice. Sometimes, the pus doesnot descend freely, maybe due to occlusion of sinus orifice by polyps.
- 12. SIGNS OF ACUTE SINUSITIS: Tenderness over the maxilla, especially in the infraorbital region. Mild edema of cheek in infraorbital soft tissues.
- 13. Rarely, patient gets earache, as a referred pain from antrum. This is attributed to acute otitis media. Percussion of maxillary premolars and molars related to affected sinus will lead to pain. Presence of pus or mucopurulent discharge in middle meatus and traclking down posterior wall of pharynx.
- 14. SIGNS AND SYMPTOMS OF CHRONIC SINUSITIS: Impairment of sense of smell Foul smelling of mucopurulent discharge Herniation of polyp into middle meatus Prolapse of polyp through the fistula
- 15. INTRAORAL EXAMINATION: Descending postnasal floor of mucopurulent discharge Herniation of polyp into middle meatus Prolapse of polyp through the fistula
- 16. If the fistula is large, it can be assessed from inspection. Nose blowing test: compression of anterior nares, followed by gentle blowing of nose (with mouth open), causes a rise in intranasal pressure exhibited by the whistling sound as air passes down the open passage. Mouth mirror test A wisp of cotton-wool held just below the alveolar opening will usually be deflected by the air stream. Patient is asked to hold fluid within the mouth, fluid can be seen escaping through the nose. Betadine can be mixed with the fluid to differentiate between nasal secretion and rinsing fluid.
- 17. PURPOSE 1. To protect the sinus from oral microbial flora 2. To prevent escape of fluid and other contents across the communication 3. To eliminate existing antral pathology 4. To establish drainage through inferior meatus A fistulous tract present for more than 14 days should be considered as a chronic fistula.
- 18. Management of oroantral communication depends on 2 factors 1. Size of communication: Small size communications heals better, Large size communication > 5mm may result in chronic oroantral fistula. 2. Preoperative condition of maxillary sinus: If maxillary sinus is infected before surgery even small communication will not heal. If patient has maxillary sinusitis OAC will heal poorly and chronic oroantral fistula results.
- 19. • Surgeon should ensure that high quality blood clot is formed in the socket. • Advise patient - sinus precautions so that clot will not dislodge. • Surgeon must not probe into sinus through socket because it may introduce foreign bodies and bacteria into sinus, it may also lacerate sinus membrane. If size of OAC is 2mm or less in diameter • Additional measures are required to maintain blood clot in the socket. • Figure of eight suture should be placed over the socket. • Some surgeon also place gel foam in the socket to enhance clotting. • Advise drugs and sinus precautions If opening is of moderate size of 2 to 6mm • Surgeon should consider repair of OAC with a flap procedure. • Most commonly used flap for small opening is buccal advancement flap. • Closure should be performed as soon as possible preferably on the same day. • Advise drugs and sinus precautions. • Maintain follow up. If size of sinus opening is 7 mm or large
- 20. • Do Not drink with a straw. • Do Not blow your nose. • Use all medications as directed. • Do Not play any wind instruments. • Do Not smoke cigarettes, pipes, or cigars. • Do Not open your mouth widely. • Avoid swimming and strenuous exercise for at least one week. • Eat a soft or liquid diet. Chew on the opposite side of your mouth as much as possible. • Continue to brush your teeth but avoid the surgical area. Rinse three times a day with warm water. • It is not uncommon to have a slight amount of bleeding from your nose for several days.
- 21. A. TREATMENT OF EARLY CASES: • Cases where oroantral communication is recent and formation of fistula is not established. •Ideal treament a. Immediate surgery repair to achieve primary closure b. Simultaneous antibiotic prophylaxis to prevent sinus infection The immediate primary closure is done by a simple reduction of the buccal and palatal socket walls, to allow coaptation of buccal and palatal tissue flaps to close over the defect. A protective acrylic denture or splint can be used to provide a barrier to the inadvertent entry of food particles.
- 22. Antibiotics: - These are used until symptoms begin to subside - It can be started with IV route and later switched over to oral route. - Pencillin V 250 to 500mg six hourly is adequate. Nasal decongestants: - These encourage the drainage of pus and secretions. - e.g. Ephedrine(0.5%) or otrivin nasal drops 3 drops/ 3times daily / 7 days -
- 23. Analgesics: -NSAIDs: 1.Aspirin 500mg 4 times daily 2. Paracetamol 500mg 3 times daily 3. Ibuprofen 400mg 3 times daily
- 24. It includes: a. Whitehead’s varnish pack : the pack is used over the socket and secured with suture Whitehead’s varnish: Benzoin 10 parts 44g Storax 7.5 parts 33g Balsam of tolu 5 parts 22g Iodoform 10 parts 55g Solvent-ether to 1 fl oz or 100 parts b. Denture plate: it is indicated when surgical repair of fistula is to be deferred. It provides barrier to prevent entry of food particles in antrum.
- 25. • Cases seen more than 24 hours after accident: - It is preferable to defer the surgical closure until the gingival edges of the fistula have healed soundly (approx 3 weeks) - Supportive measures should be given - Maxillary sinus should be gently irrigated with warm normal saline, if there is purulent discharge or signs of acute or chronic sinusitis is seen. • Cases of long duration(more than a month): - Surgical closure is required
- 26. Depending upon the type of flap used it can be divided into three groups: Buccal flap Palatal flap Combination of both
- 30. It is performed to facilitate the drainage at the conclusion of an operation performed: i. To close an oro-antralfistula, or ii. To remove a tooth or a root from sinus. Drawbacks: It is a controversial surgical procedure for the following reasons: (i) It cannot drain the sinus, satisfactorily; as the point created for drainage is not at the point of dependent drainage; due to the fact that antral floor is about 1.5 cm below nasal floor, (ii) It also interferes with ciliary pathways: thus impedes normal physiological drainage of sinus.
- 31. Surgical Procedure for Intranasal Antrostomy i. A small-sized osteotome or gouge is pushed through the inferior meatus in the nasal cavity, into the maxillary sinus. Then a big curved artery forceps is passed through this opening and a iodoform impregnated ribbon gauze pack’s end is grasped into its beak and pulled out into the nostril. Here a single knot, which is put in the ribbon gauze will help to keep it secured in the nostril. The other end of the ribbon gauze is then used to systematically pack the maxillary sinus cavity in multiple folds, after achieving proper hemostasis (after Caldwell- Luc operation).
- 32. ii. An antrostomy can be performed by removing approximately 1 cm of the medial wall of the antrum, which bulges into the sinus below the level of the inferior turbinate. This antrostomy should be extended to the level of the floor of the nose. The nasal mucosa is then incised from the antral surface on three sides and the nasal mucosal flap thus created is reflected into the antrum.
- 34. Flap design Palpation of bony edge
- 35. Excising the fistula and reflect the flap
- 37. Palatal reversal & buccal advancement flap
- 38. Functional Endoscopic Sinus Surgery Caldwel-Luc procedure Lateral Rhinotomy
- 39. • Purpose - To restore normal paranasal air sinuses mucociliary function • Indications - Recurrent sinusitis with steanosis at the osteomeatal unit - Chronic hyperplastic sinusitis with obstructive nasal polyp - Chronic sinusitis with mucocele formation - Neoplasms - Orbital celllulitis/abscess unresponsiveness to medical treatment
- 40. •Relative Indications (i) Repair of cerebral spinal fluid leaks (ii)Selectednasofrontal recess/frontal sinus mucoceles (iii)Orbital decompression in bilateral exophthalmos (iv)Sinusmediated cephalagia
- 41. • This is the classic operation used when medical therapy fails to treat maxillary sinusitis effectively or when an open surgical approach is needed to treat a cyst or tumor of maxillary sinusitis • Caldwell in 1893 & Henri Luc in 1897
- 42. 1. Open procedure for removal of root fragments, teeth or foreign body or an antrolith (stone) from the maxillary sinus. 2. To treat chronic maxillary sinusitis with hyperplastic lining and polypoid degeneration of the mucosa. 3. Removal of cysts or benign growths from the maxillary sinus. 4. Management of hematoma in the maxillary sinus and to control post traumatic hemorrhage in the sinus. 5. Zygomaticomaxillary complex fractures involving floor of the orbit and anterior wall of the maxillary sinus. 6. Removal of impacted canine or impacted third molar. 7. Along with closure of chronic oroantral fistula, associated with chronic maxillary sinusitis.
- 43. • Under LA with sedation or under GA • A semilunar incision is planned in the buccal vsetibule from canine to 2nd molar, just above the gingival attacment. • A mucoperiosteal flap is elevated • An opening or window is created in the anterior wall of maxillary sinus.
- 44. • It is then enlarged in all directions with Rongeur forceps, to permit the inspection of sinus cavity. • Pus should be sucked away and thorough irrigation of maxillary sinus is carried out with copious saline wash. • Removal of root, tooth gauze, bone wax or stone is done • The thickened, infected lining of the sinus can be elevated with Howarths periosteal elevator and removed and sent for histopathology
- 45. • In case of profuse bleeding- sinus is packed with ribbon gauze soaked in adrenaline 1:1000 for 1 or 2 minutes • The antral cavity is irrigated again and can be packed with iodoform ribbon gauze. • The incison is closed with 3-0 silk
- 46. Indication • well differentiated or low grade tumor such as inverted papillomas tumors of limited extend on the lateral wall of nasal cavity or medial wall of the antrum
- 47. Textbook Of Oral And Maxillofacial Surgery; 4th Edition; Prof. Dr. Neelima Anil Malik.
Editor's Notes
- VALSALVA TEST: To confirm if OAC has occurred The Valsalva manoeuvre is performed by moderately forceful attempted exhalation against a closed airway, usually done by closing one's mouth, pinching one's nose shut while pressing out as if blowing up a balloon. Oroantral communication can also be confirmed by observing the passage of air or bubbling of blood from the post-extraction alveolus when the patient tries to exhale gently through their nose while their nostrils are pinched. If the patient exhales through their nose with great pressure, there is a risk of causing oroantral communication, even though communication may not have occurred initially, such as when only the mucosa of the maxillary sinus is present between the alveolus and the antrum