This document discusses dento-alveolar infections, including:
- The stages of inflammation and types of irritants that can cause infections.
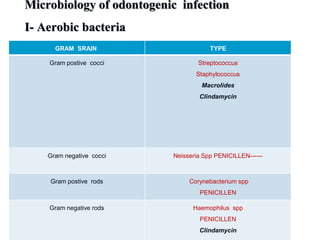
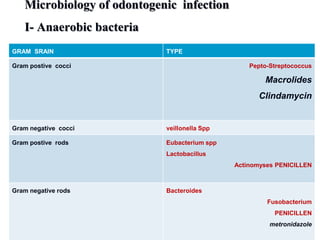
- The bacteria commonly found in oral infections and the environments they thrive in.
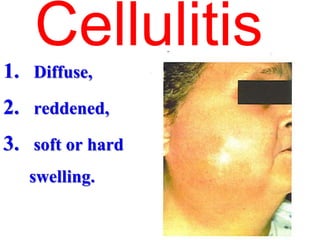
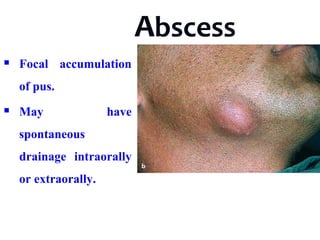
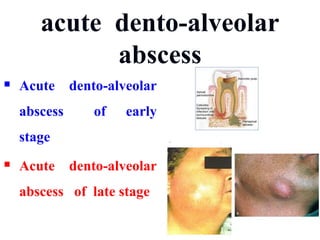
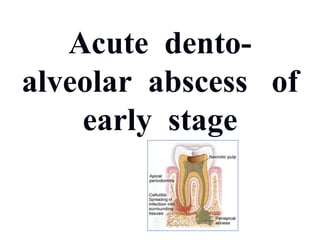
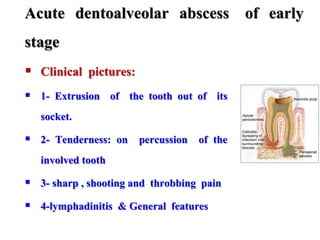
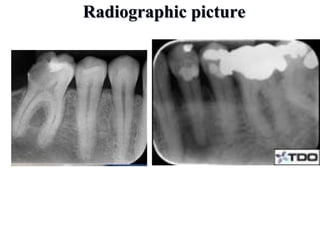
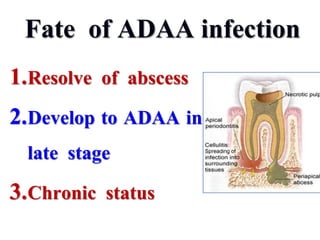
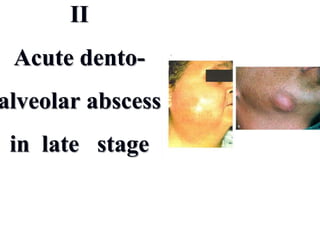
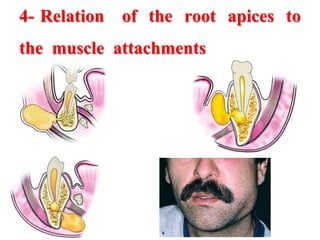
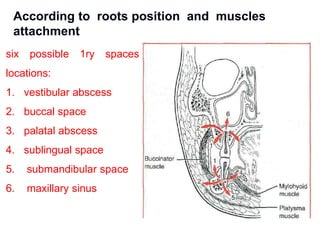
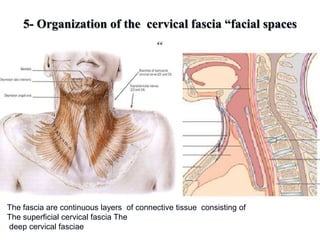
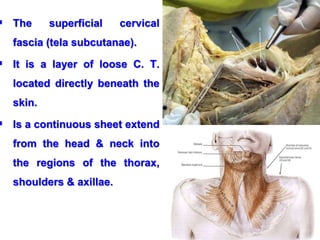
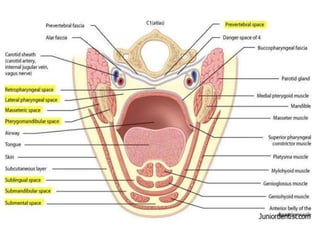
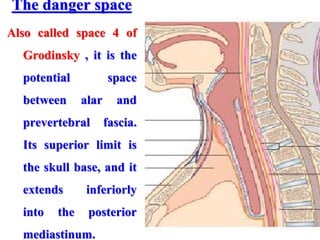
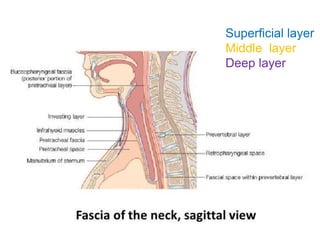
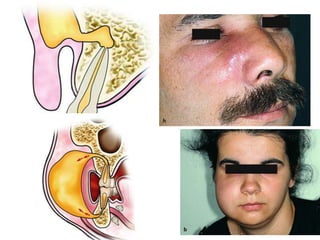
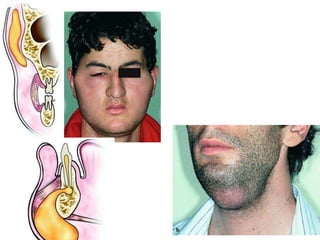
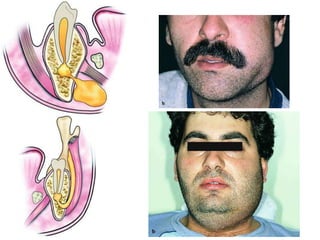
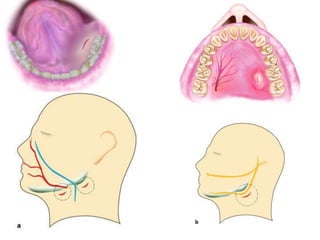
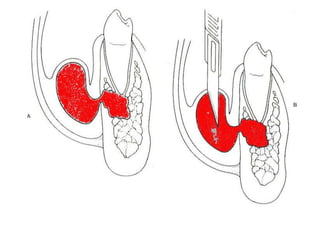
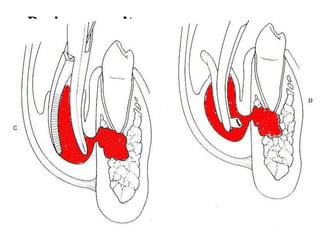
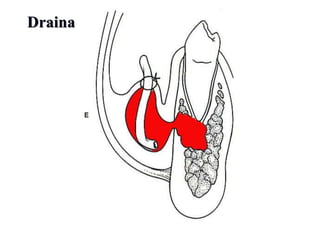
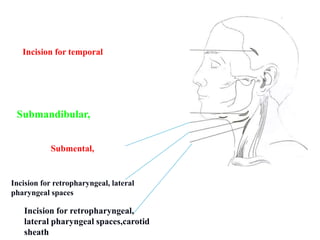
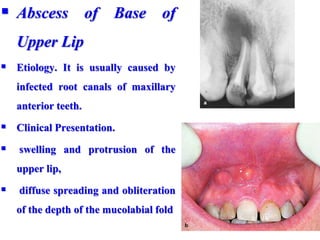
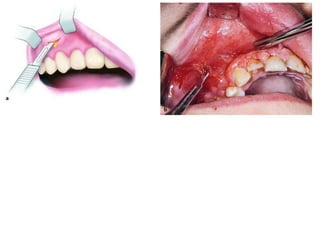
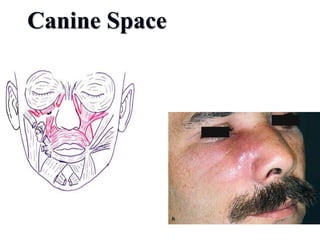
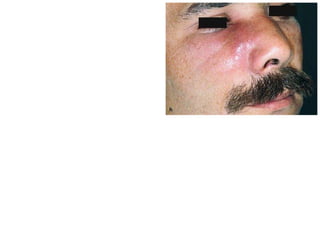
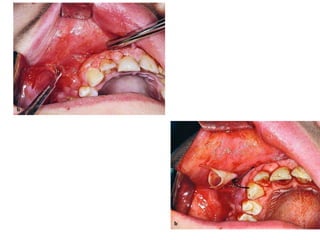
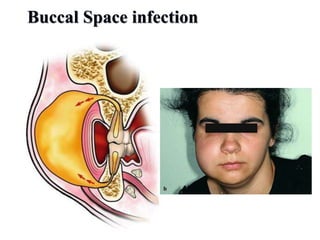
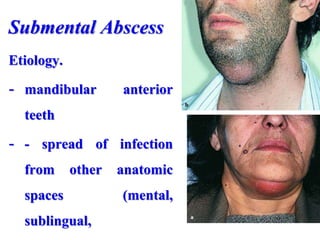
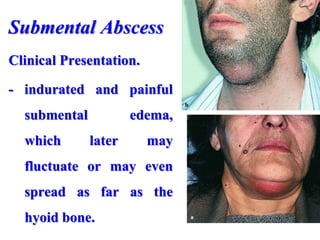
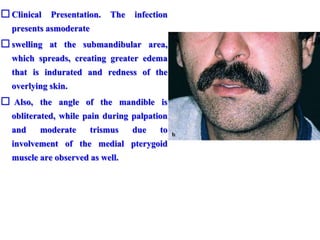
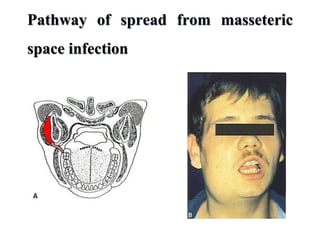
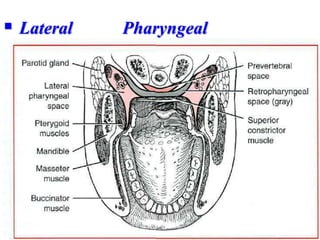
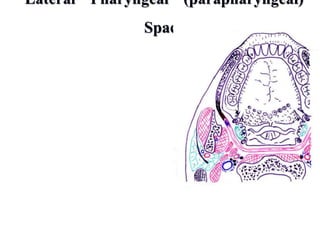
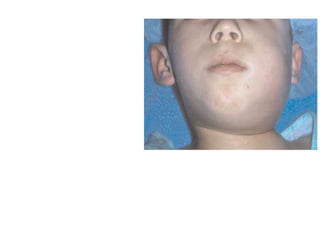
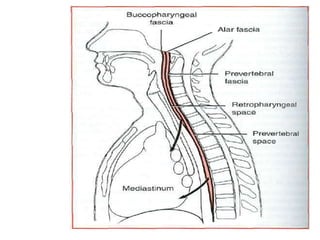
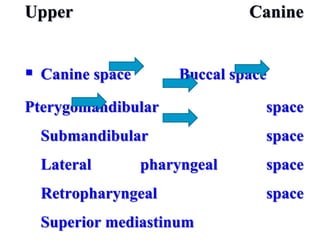
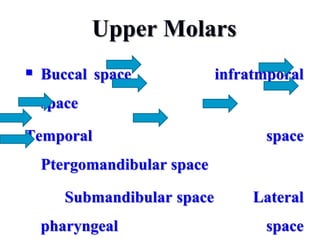
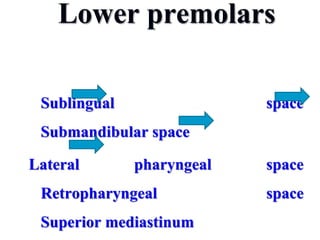
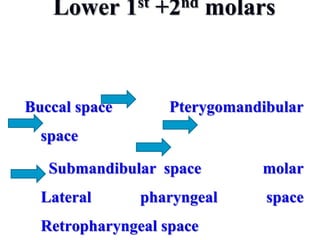
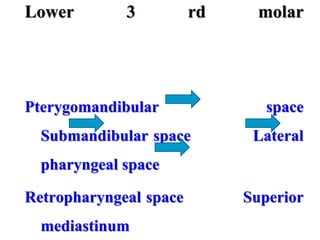
- The progression of odontogenic (tooth-related) infections from early to late stages and the spread of infection through facial spaces.
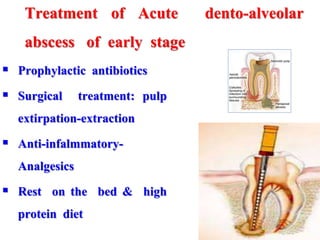
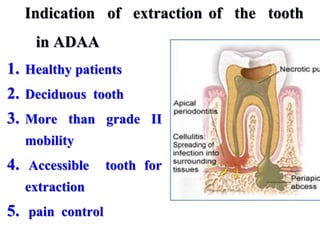
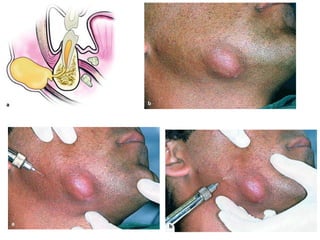
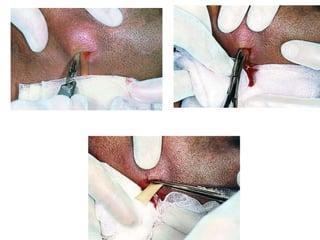
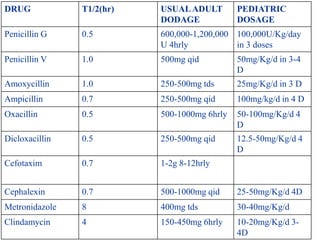
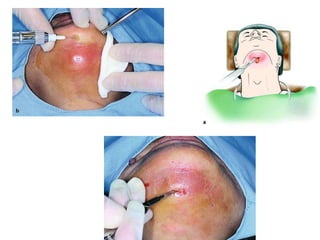
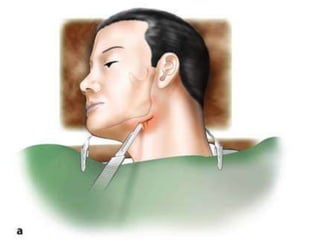
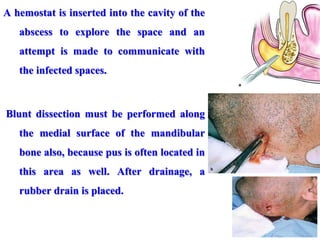
- The principles of diagnosing and managing odontogenic infections, including determining severity, evaluating the host, surgical drainage, antibiotic therapy, and frequent evaluation of the patient.