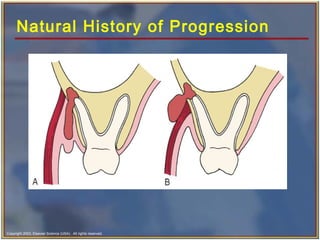
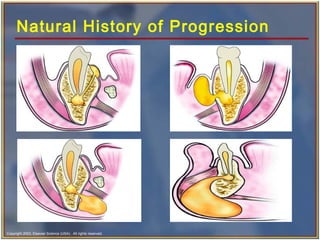
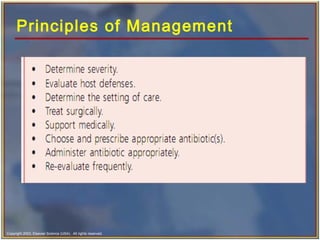
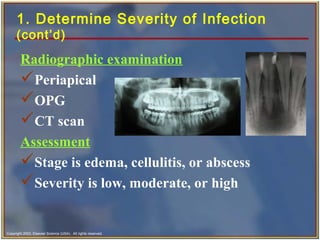
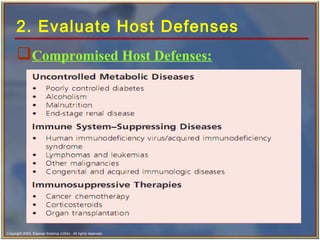
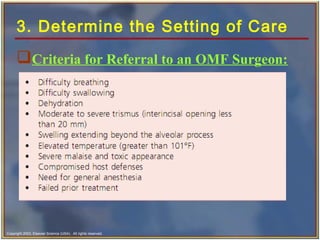
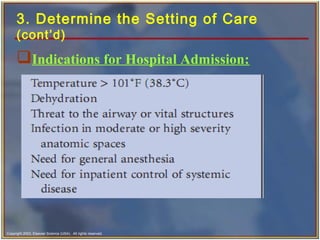
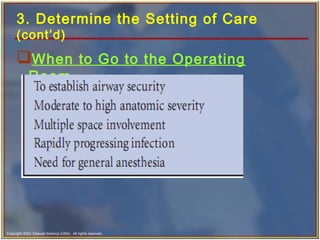
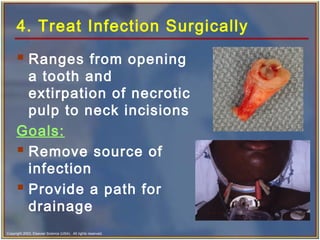
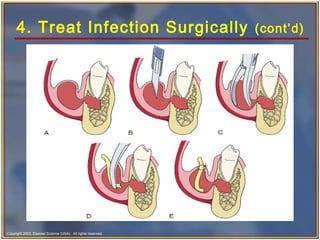
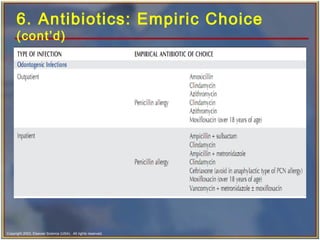
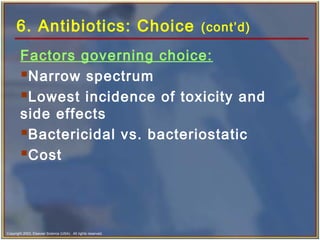
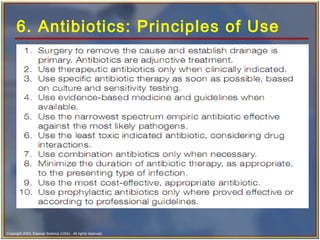
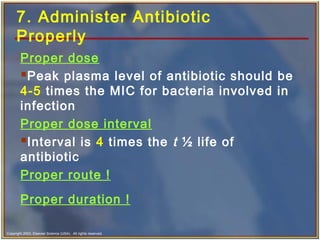
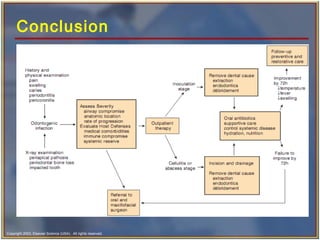
This document discusses the principles of managing odontogenic infections. It covers the etiology, microbiology, natural progression, and 8 principles of therapy: 1) determine severity, 2) evaluate host defenses, 3) determine setting of care, 4) treat surgically, 5) support medically, 6) choose and prescribe antibiotics, 7) administer antibiotics properly, and 8) evaluate the patient frequently. The document provides details on each principle, including which bacteria commonly cause infections, appropriate antibiotic choices, and factors in determining treatment setting.