The document discusses the motor control system of the human brain, particularly focusing on the roles of different areas of the cerebral cortex, including primary motor areas and various specialized areas involved in voluntary movement planning and execution. It covers the integration of information from sensory areas, subcortical structures, and the spinal cord, stressing the importance of functional overlap between cortical areas and the consequences of motor lesions. Additionally, it delves into specific speech and writing deficits related to damage in certain regions like Broca's area and Exner's area, classifying different types of aphasia caused by such lesions.
![Cerebral cortex
• Cerebral cortex is the highest centre of
brain.
• It has a total surface area 0.2-0.25 m of
which about one third is exposed.
• The total cerebral cortex contain 100 billion
neurons.
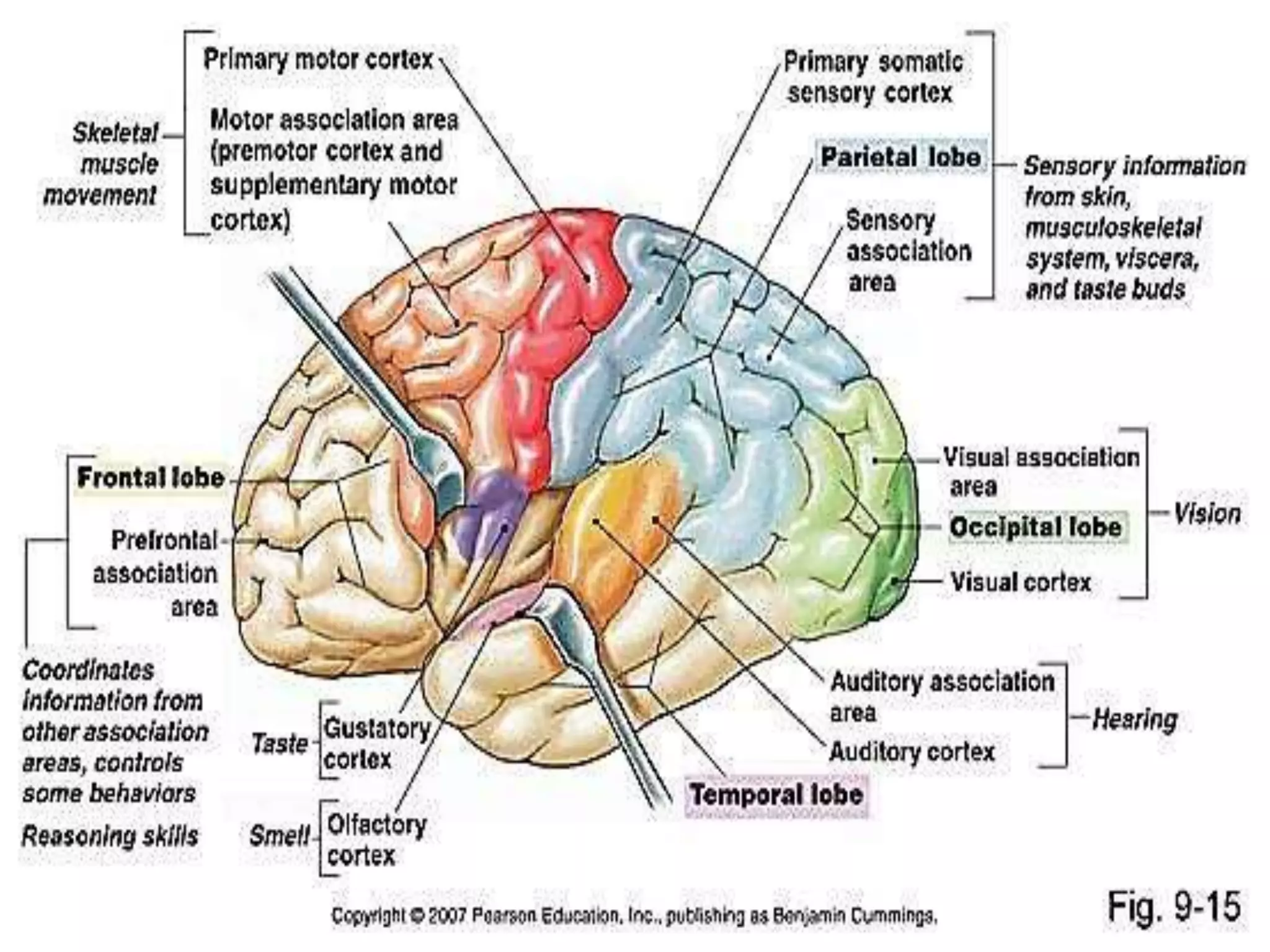
It is divided by mean of primary fissures into
[frontal, parietal ,temporal,occipital,limbic
lobe]
It is divided by mean of secondary fissures
into gyri [eg. post central gyrus]](https://image.slidesharecdn.com/project211-150228125116-conversion-gate02/75/motor-areas-of-cerebral-cortex-4-2048.jpg)