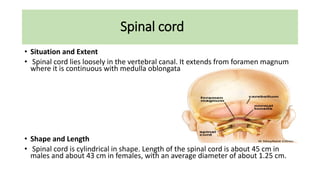
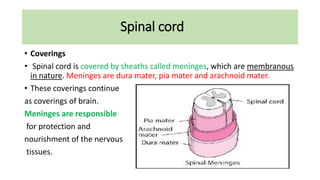
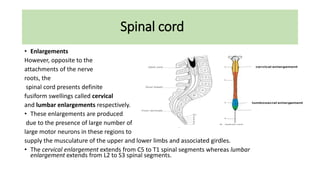
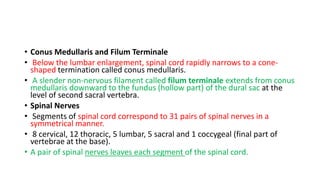
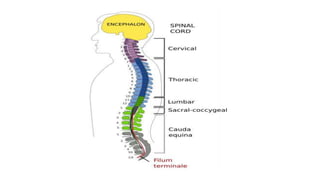
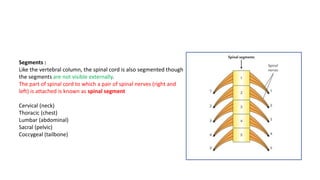
The document summarizes key aspects of the spinal cord's anatomy and function. It describes the spinal cord's location, shape, length, coverings, enlargements, internal structure including grey and white matter, segments, and tracts. It also outlines some of the spinal cord's major functions, including electrochemical communication, enabling walking through coordinated muscle contractions, and facilitating reflexes through involuntary responses between the brain, spinal cord and peripheral nerves.

































![2-Anatomy of the Spinal Cord [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/2-anatomyofthespinalcordautosaved-240314080102-4f8095d0-thumbnail.jpg?width=640&height=640&fit=bounds)

























































