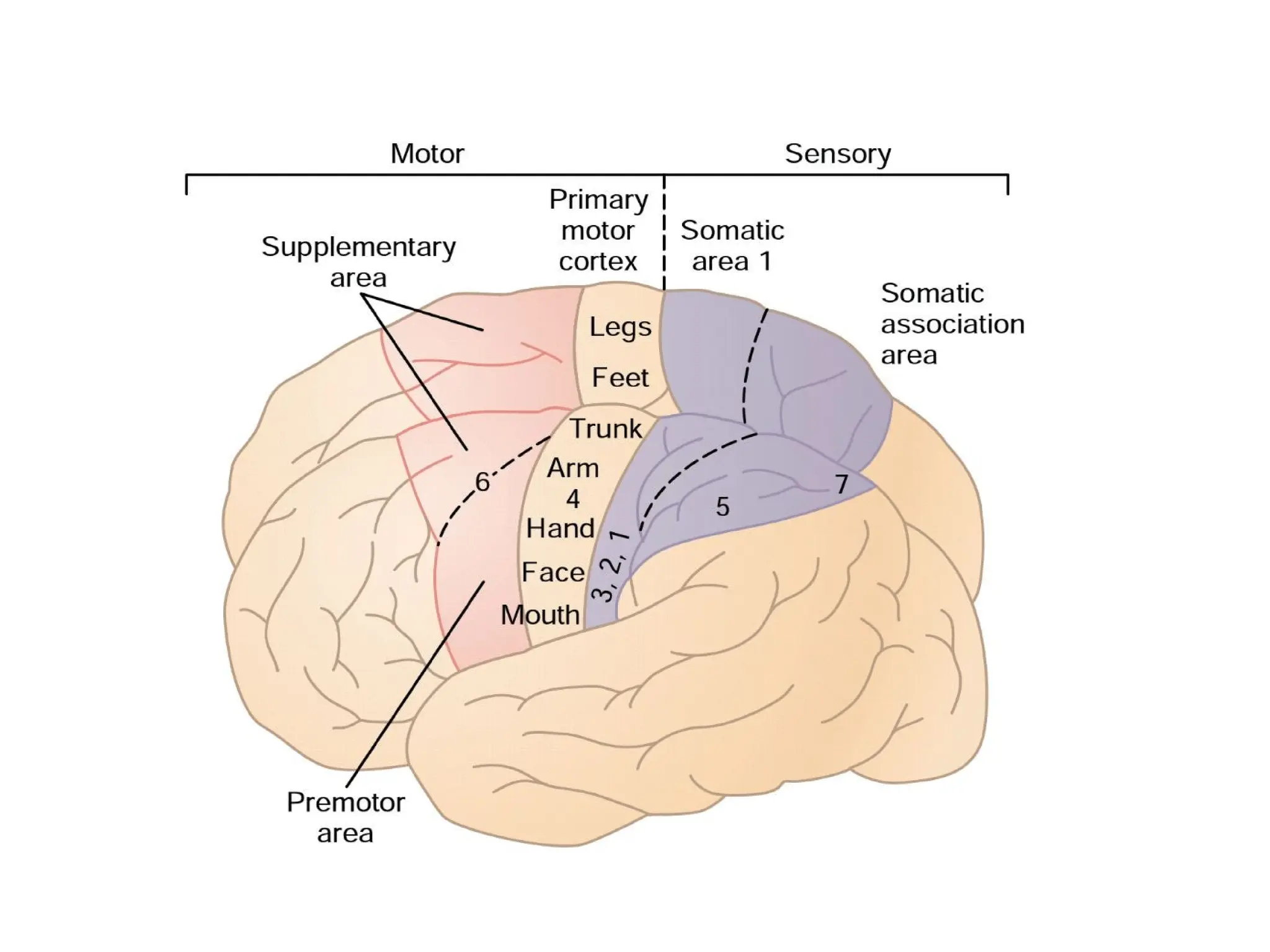
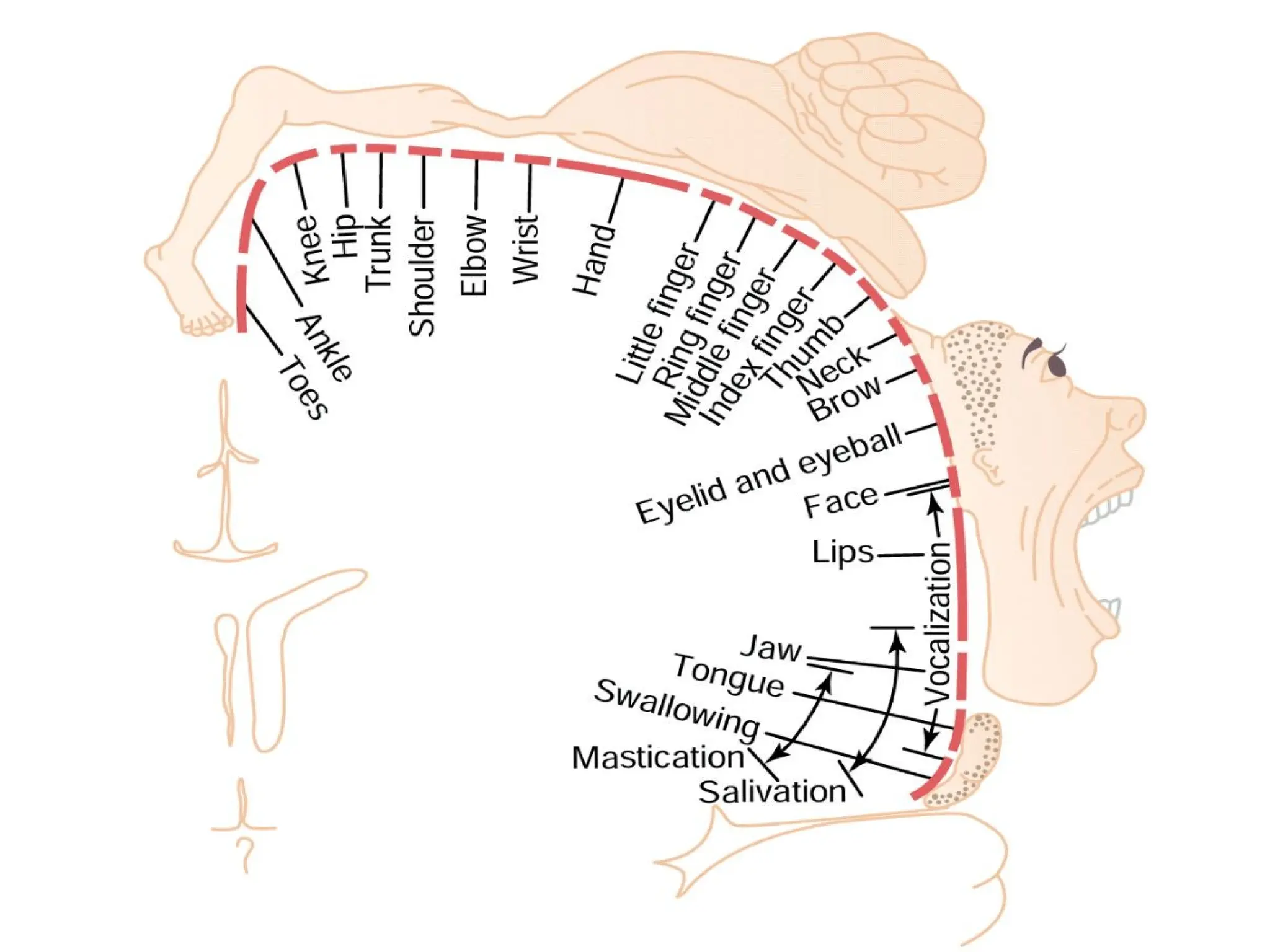
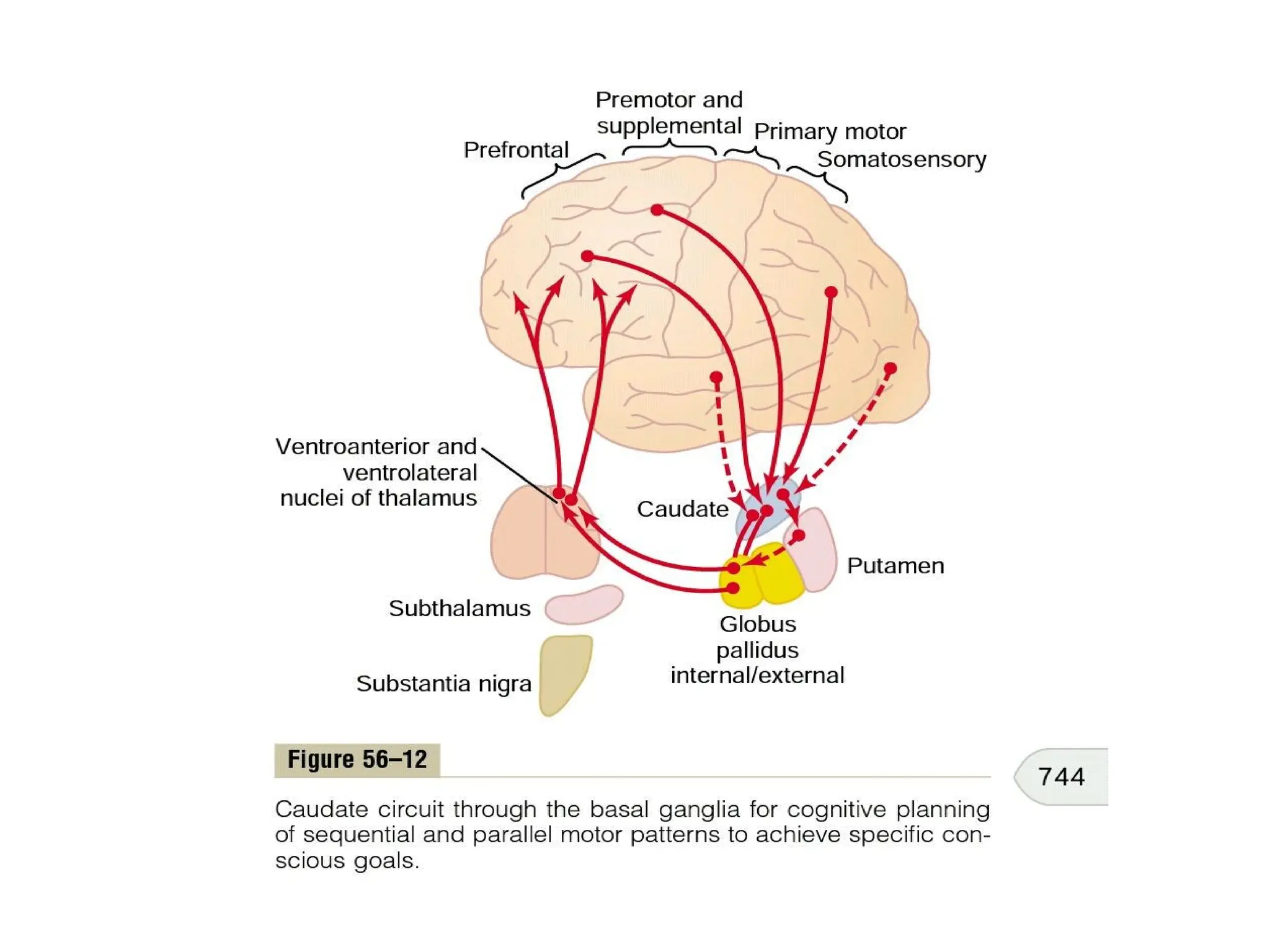
The document discusses the intricate control of motor functions in the brain, emphasizing the roles of the motor cortex, brain stem, cerebellum, and basal ganglia in facilitating voluntary movements. It details the organization of motor pathways, the nature of motor signals, and the consequences of lesions in these areas, outlining various motor control systems and the functions of specific regions like Broca's area and the semicircular ducts. Additionally, it describes how the brain integrates sensory feedback to maintain motor coordination and equilibrium.








![Neurological assessmentv1[25 10_11][1]](https://cdn.slidesharecdn.com/ss_thumbnails/neurological-assessmentv1-5b25-10-11-5d-5b1-5d-130511142954-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)






































