Downloaded 592 times

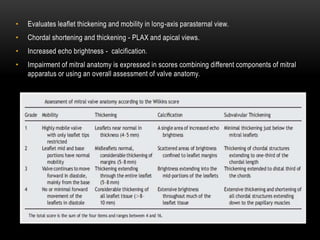

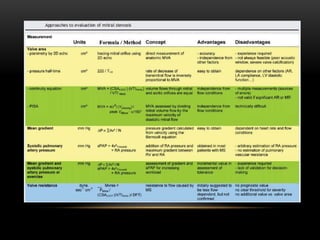

Echocardiography is a key tool for diagnosing and evaluating mitral stenosis (MS). It is essential to use an integrative approach when grading MS severity by combining Doppler, 2D imaging, and measurements, rather than relying on one alone. Echocardiography plays a major role in MS by confirming diagnosis, quantifying severity, analyzing consequences, and examining valve anatomy. Mitral valve planimetry directly measures valve area and is considered the reference standard, but additional measurements like pressure gradient and half-time are also useful. Echocardiography aids clinical decision making for patients with MS.























































































