Downloaded 909 times




![• In healthy adults, aortic diameters do not usually
exceed 40 mm and taper gradually downstream.
• They are variably influenced by several factors
including age, gender, body size [height, weight, body
surface area (BSA)] and blood pressure.
• In this regard, the rate of aortic expansion is about 0.9
mm in men and 0.7 mm in women for each decade of
life.
• This slow but progressive aortic dilation over mid-to-
late adulthood is thought to be a consequence of
ageing, related to a higher collagen-to-elastin ratio,
along with increased stiffness and pulse pressure.](https://image.slidesharecdn.com/aorticaneurysmfinal-170703194412/75/Aortic-aneurysm-final-5-2048.jpg)




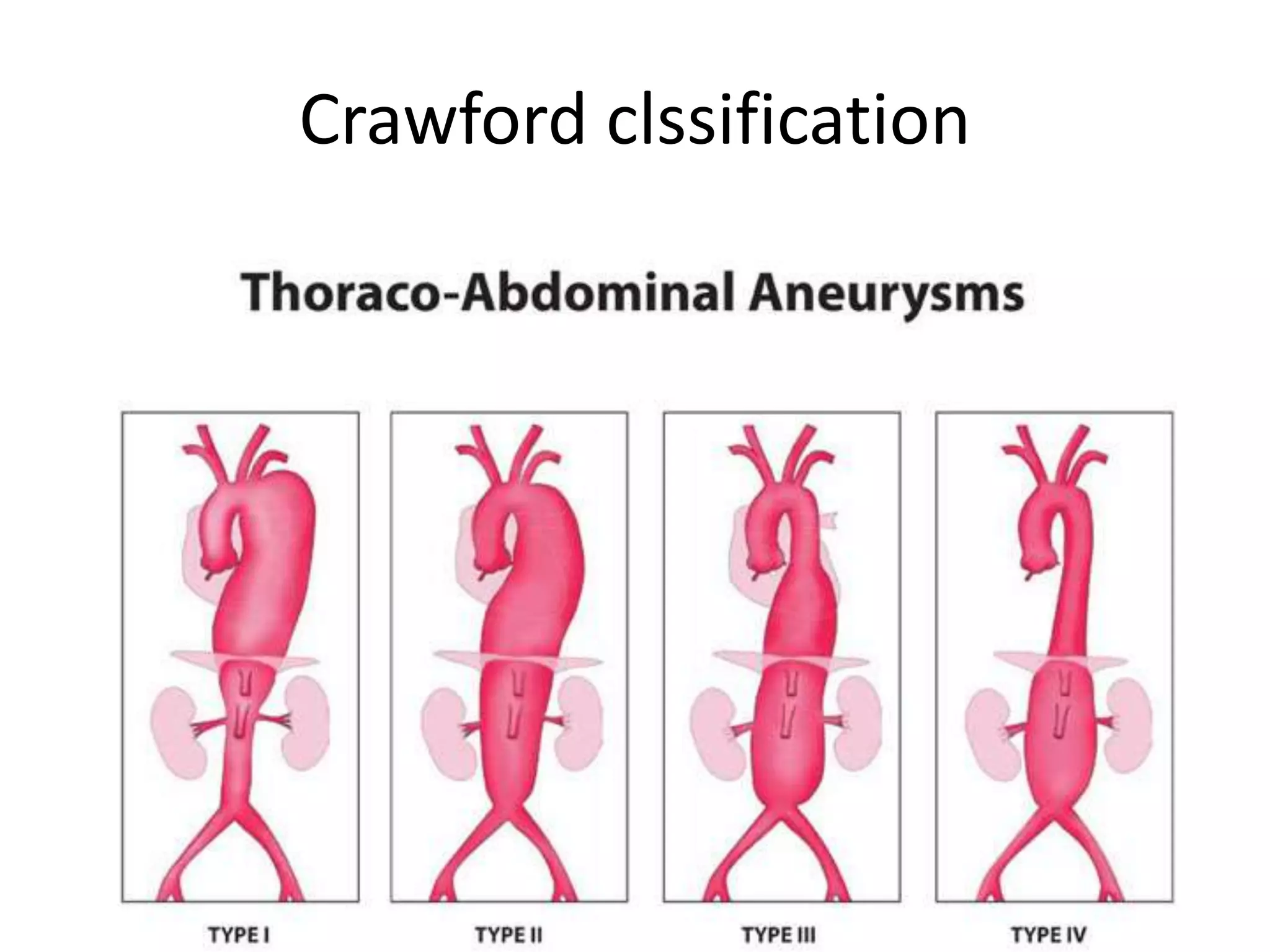






































































This document discusses aortic aneurysms, including their anatomy, physiology, risk factors, diagnosis, and management. It provides details on: 1) The layers of the aortic wall and how they give the aorta elasticity and strength. 2) Factors that cause the aortic wall to stiffen with age like increases in collagen and calcification of elastic fibers. 3) Definitions of aortic aneurysm and classifications based on location and shape. Thoracic aortic aneurysms involve the ascending aorta while abdominal aortic aneurysms are infrarenal. 4) Screening recommendations, diagnosis using imaging like ultrasound, CT and echocardiography, and considerations for open surgical repair









































































