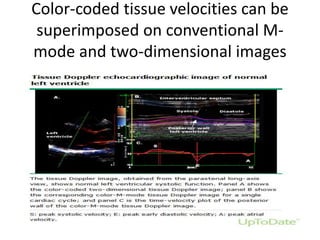
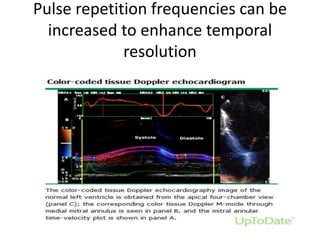
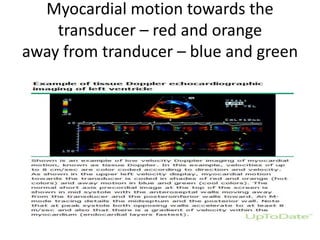
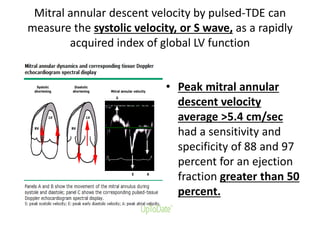
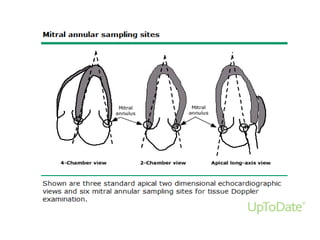
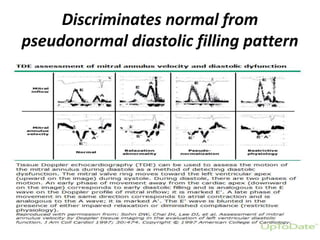
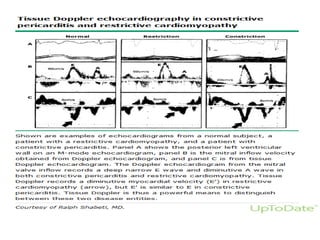
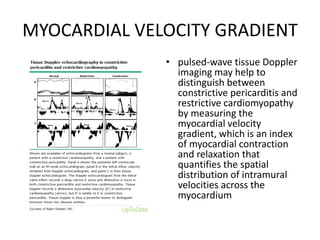
Tissue Doppler echocardiography allows assessment of myocardial motion using Doppler ultrasound. It uses frequency shifts of ultrasound waves to calculate myocardial velocity, focusing on lower velocities than blood flow Doppler. There are two techniques: pulsed TDE uses a sample volume gate while color-coded TDE uses autocorrelation to display multigated velocity data superimposed on images. TDE is useful for evaluating systolic and diastolic left ventricular function by measuring velocities of the mitral annulus, and can help distinguish conditions like constrictive pericarditis from restrictive cardiomyopathy.