This document discusses the echocardiographic evaluation of hypertrophic obstructive cardiomyopathy (HCM). Key points include:
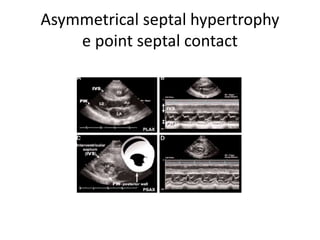
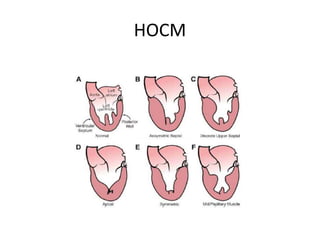
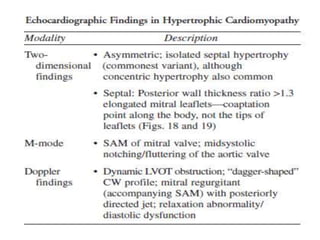
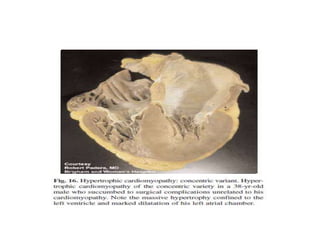
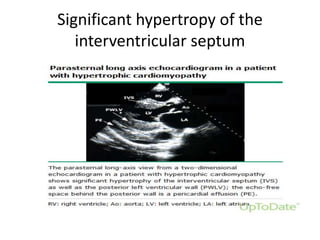
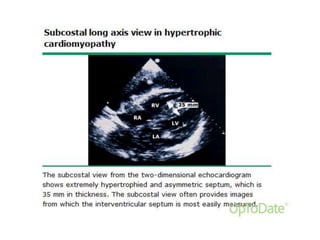
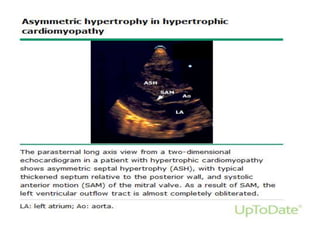
- Echocardiography is used to diagnose HCM based on unexplained left ventricular hypertrophy and rule out other causes. Asymmetric septal hypertrophy is a characteristic pattern.
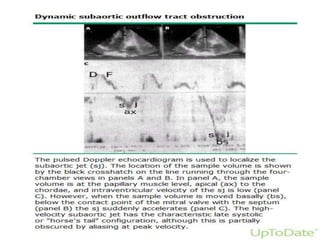
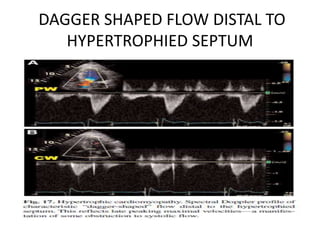
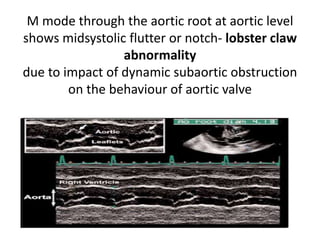
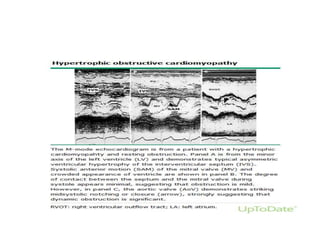
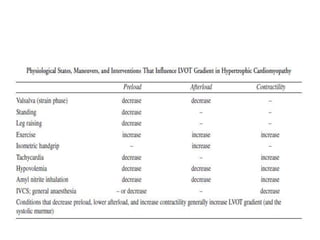
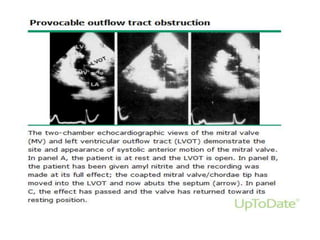
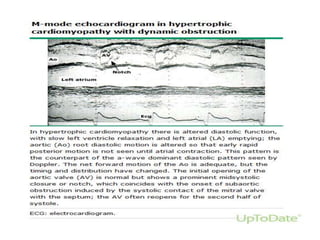
- Doppler echocardiography is used to detect left ventricular outflow tract obstruction at rest and with provocative maneuvers like Valsalva.
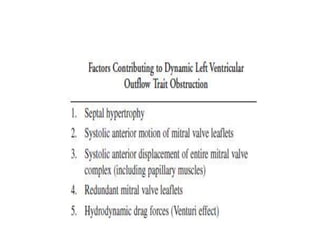
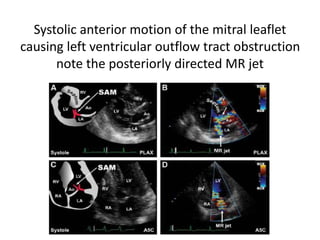
- Features like systolic anterior motion of the mitral valve indicate dynamic obstruction and need to be monitored with maneuvers.
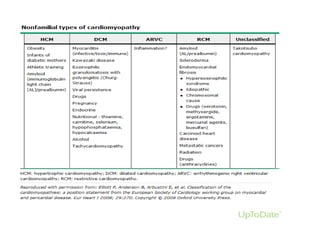
- Differential diagnosis includes secondary causes of left ventricular hypertrophy from things like hypertension which present differently on echocard











































































![Myocardial infarction [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/myocardialinfarctionautosaved-210125122422-thumbnail.jpg?width=640&height=640&fit=bounds)



















