Downloaded 8,420 times



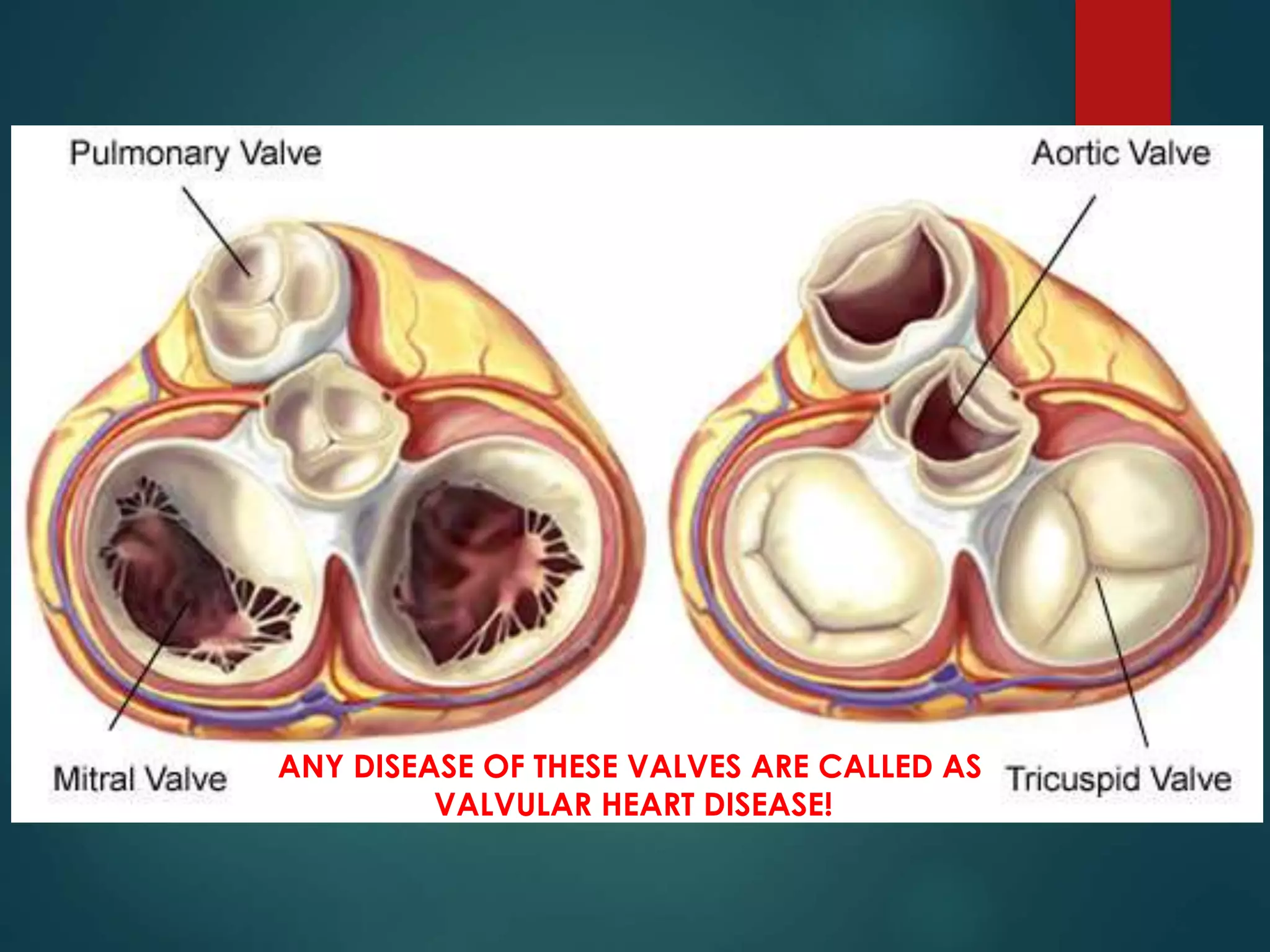
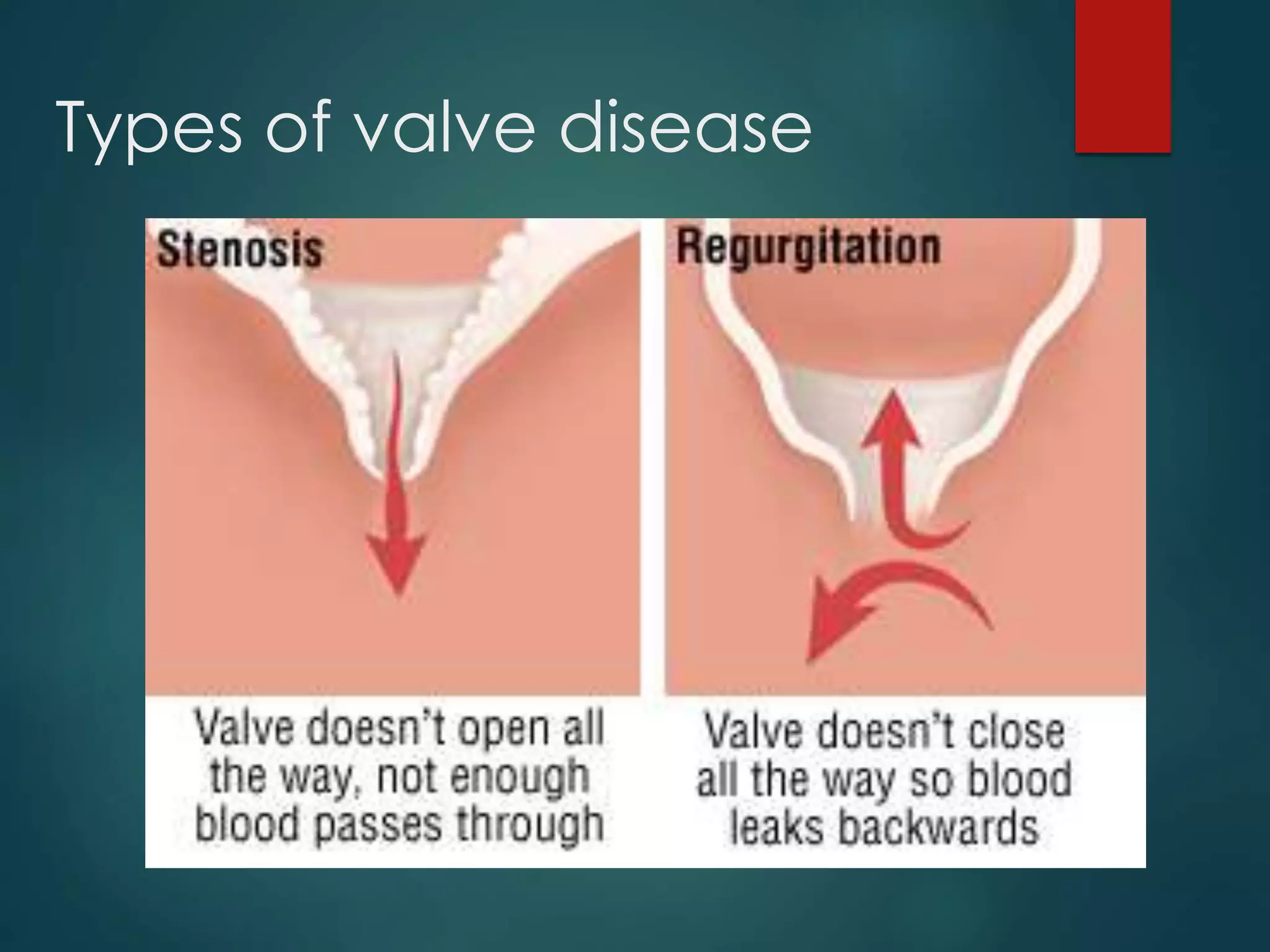













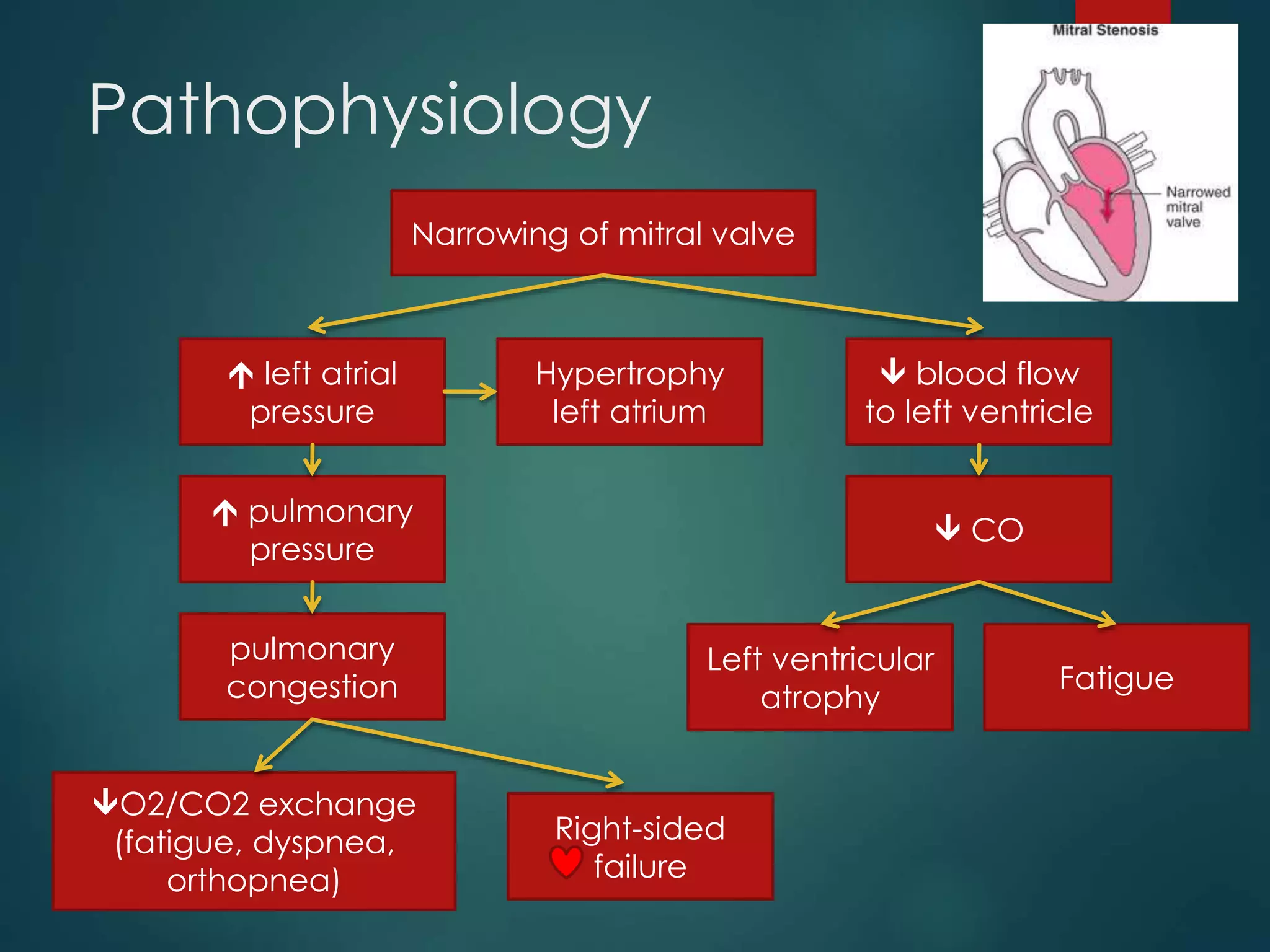










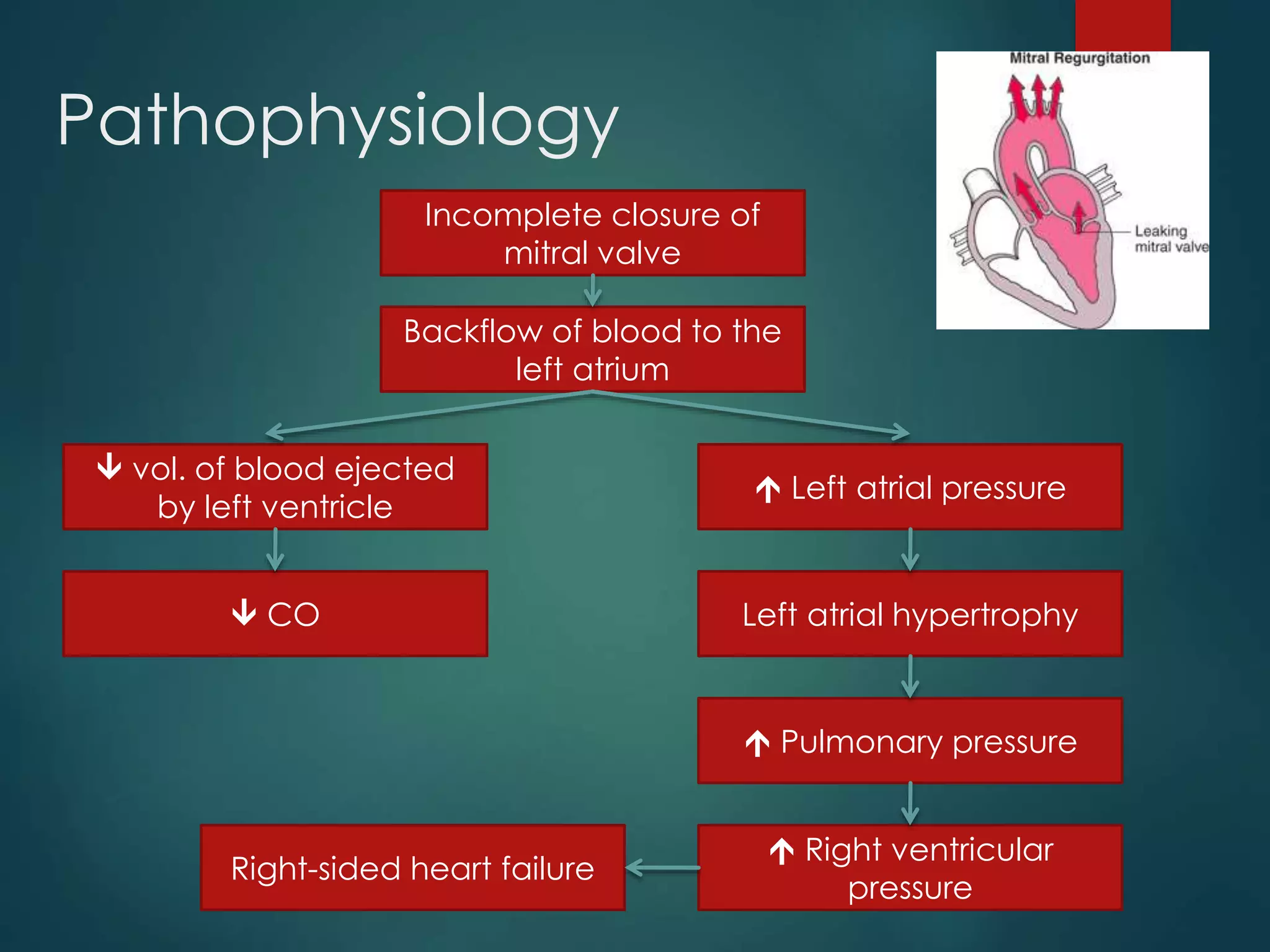










































Valvular heart disease involves heart valves not functioning properly, affecting blood flow. Common types include valvular stenosis (narrowing of valve openings) and valvular regurgitation (backflow of blood), with various causes such as rheumatic fever and congenital defects. Management may involve medical therapies, surgical interventions like valve replacement, and monitoring for complications.











































































































