Downloaded 13 times




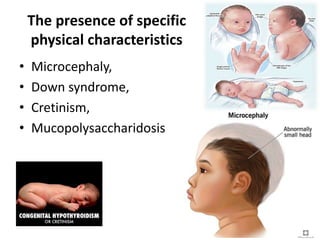




The document provides an overview of mental retardation, now referred to as intellectual disability, detailing its definitions, classifications based on IQ levels, etiology, clinical manifestations, diagnostic evaluations, and management strategies. It outlines various factors contributing to the condition, including genetic syndromes and environmental influences, as well as the importance of early intervention and specialized educational arrangements. The document emphasizes the significance of prevention methods, including genetic counseling and good maternal health, to mitigate risks associated with mental retardation.























































































