This document discusses mental retardation, including its classification, definition, causes, diagnosis, prevention, and care. Some key points:
- Mental retardation is classified based on severity from mild to profound. It is defined as subaverage intellectual functioning and deficits in adaptive skills that manifest before age 18.
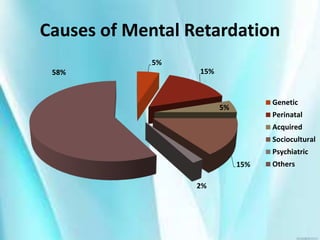
- The leading causes are genetic factors (5%), complications during pregnancy/childbirth (15%), socioeconomic deprivation (15%), and unknown factors (58%).
- Diagnosis involves assessing intellectual functioning, adaptive skills, and ruling out other conditions through tests, exams, and medical history.
- Prevention strategies include genetic counseling, prenatal care, early detection/treatment, and rehabilitation services tailored to needs. Care requires












































![Revised -ppt of child psychiatric problems [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pptofchildpsychiatricproblemsautosaved-240926091227-d0592556-thumbnail.jpg?width=640&height=640&fit=bounds)

































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)

