
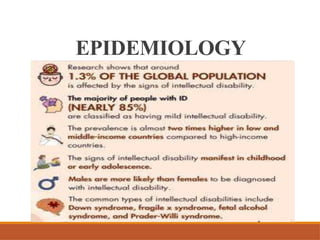





The document discusses intellectual disability (ID), previously known as mental retardation, which is characterized by below-average intelligence and challenges in daily living skills. It provides an overview of the classifications from mild to profound ID, associated causes, and various challenges faced by individuals and their families. Additionally, it emphasizes the importance of prevention, early detection, and tailored support programs for effective rehabilitation and skill development.



































![Revised -ppt of child psychiatric problems [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pptofchildpsychiatricproblemsautosaved-240926091227-d0592556-thumbnail.jpg?width=640&height=640&fit=bounds)



















































