Downloaded 61 times
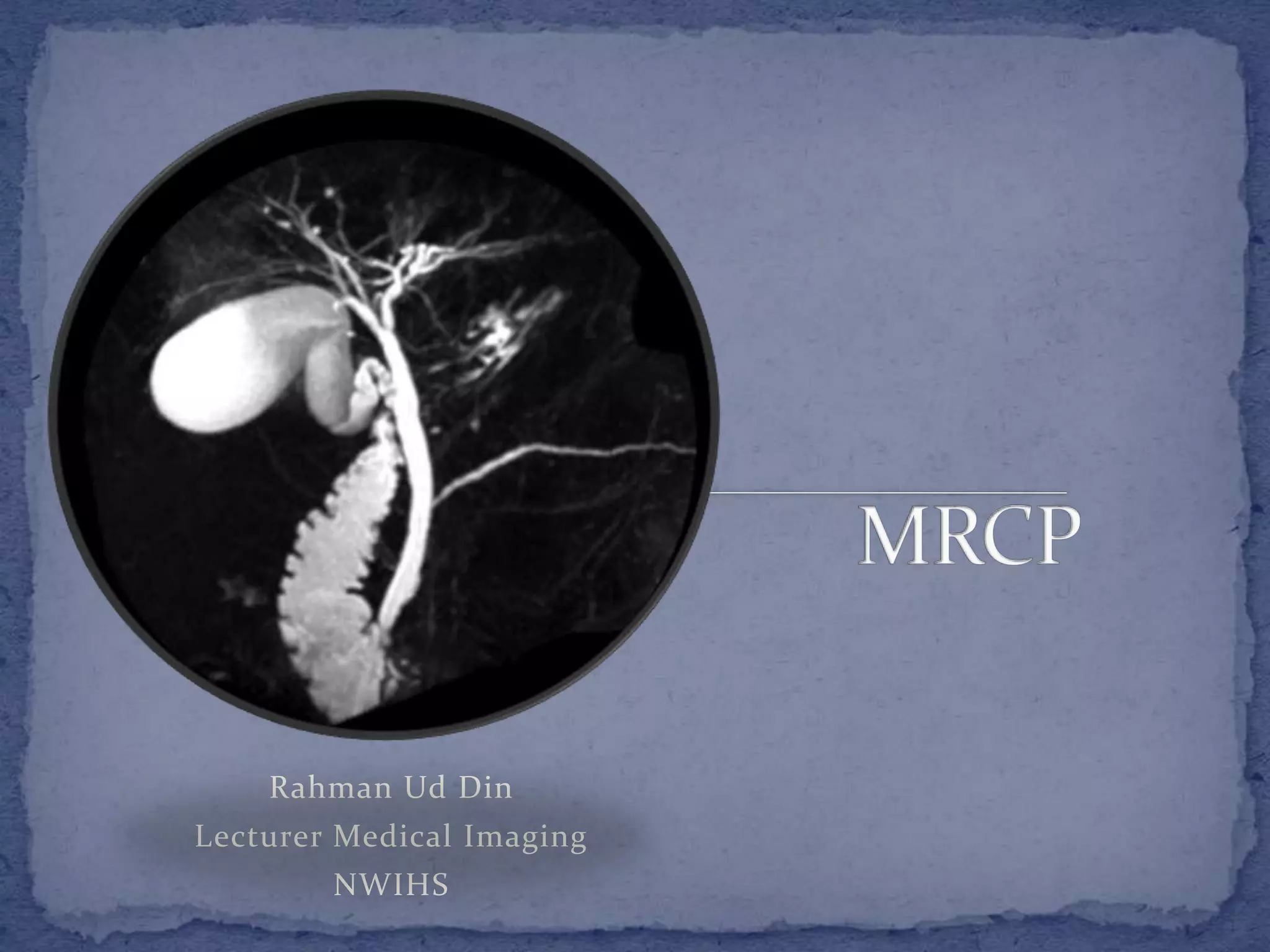



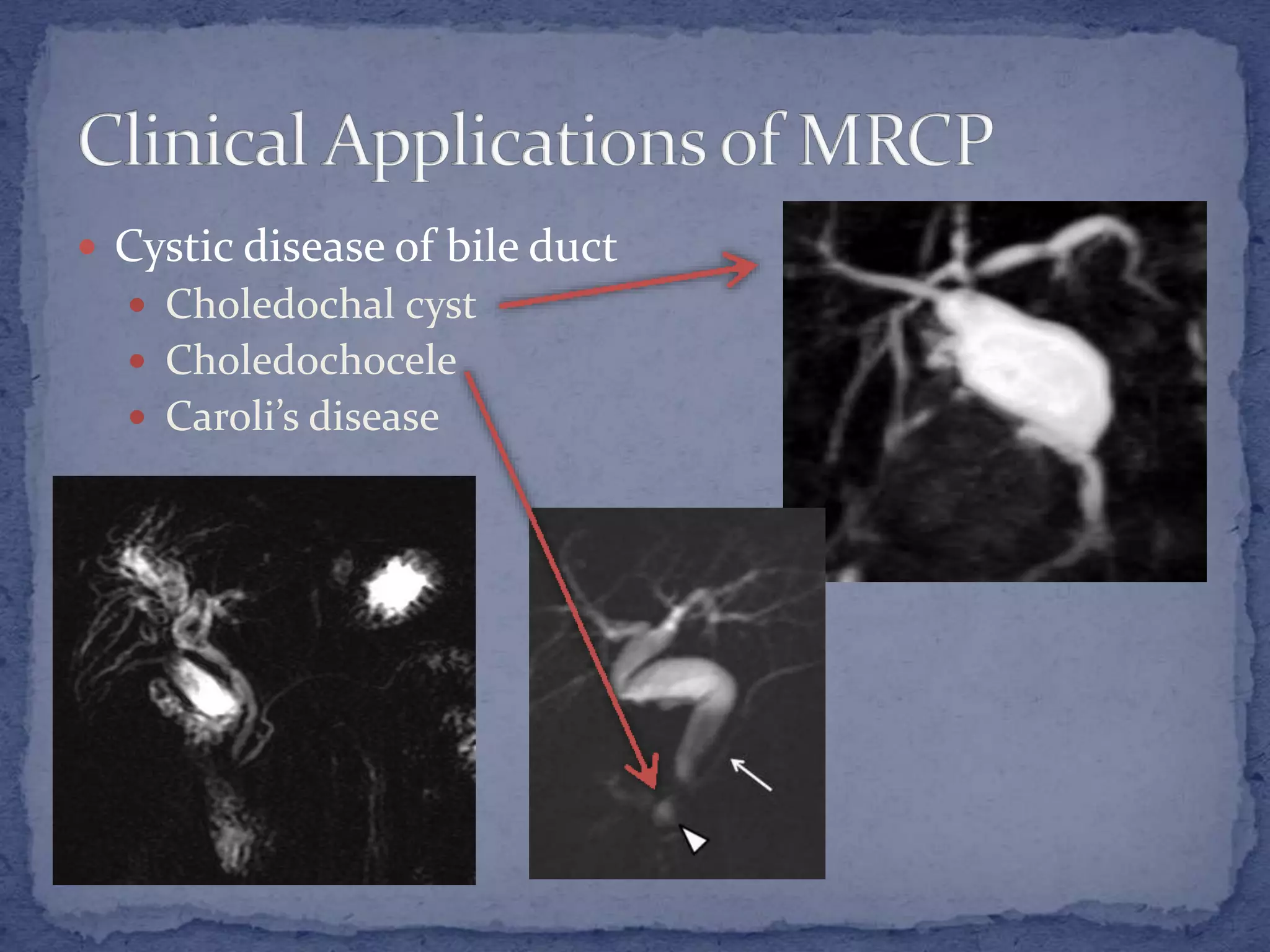

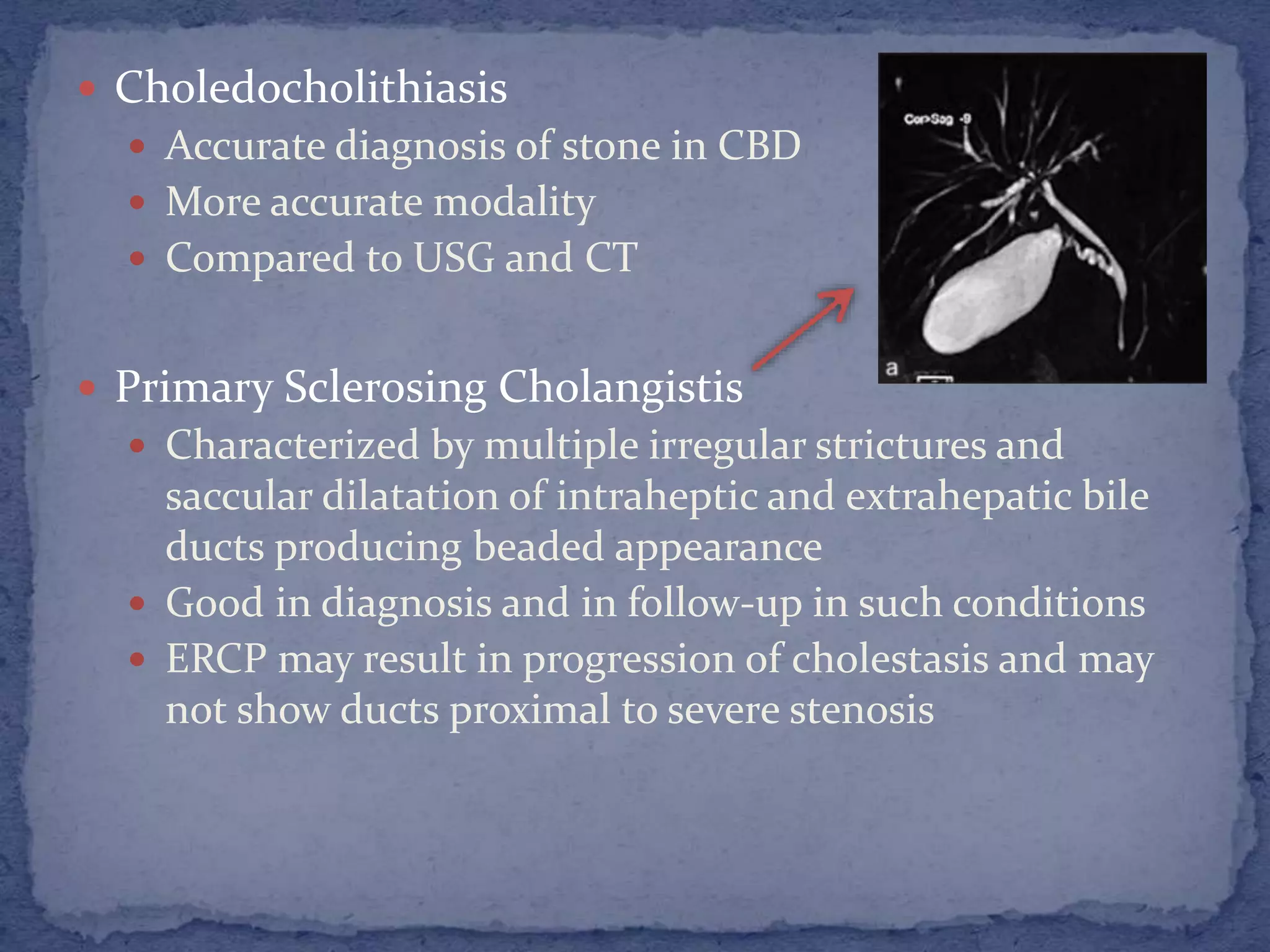
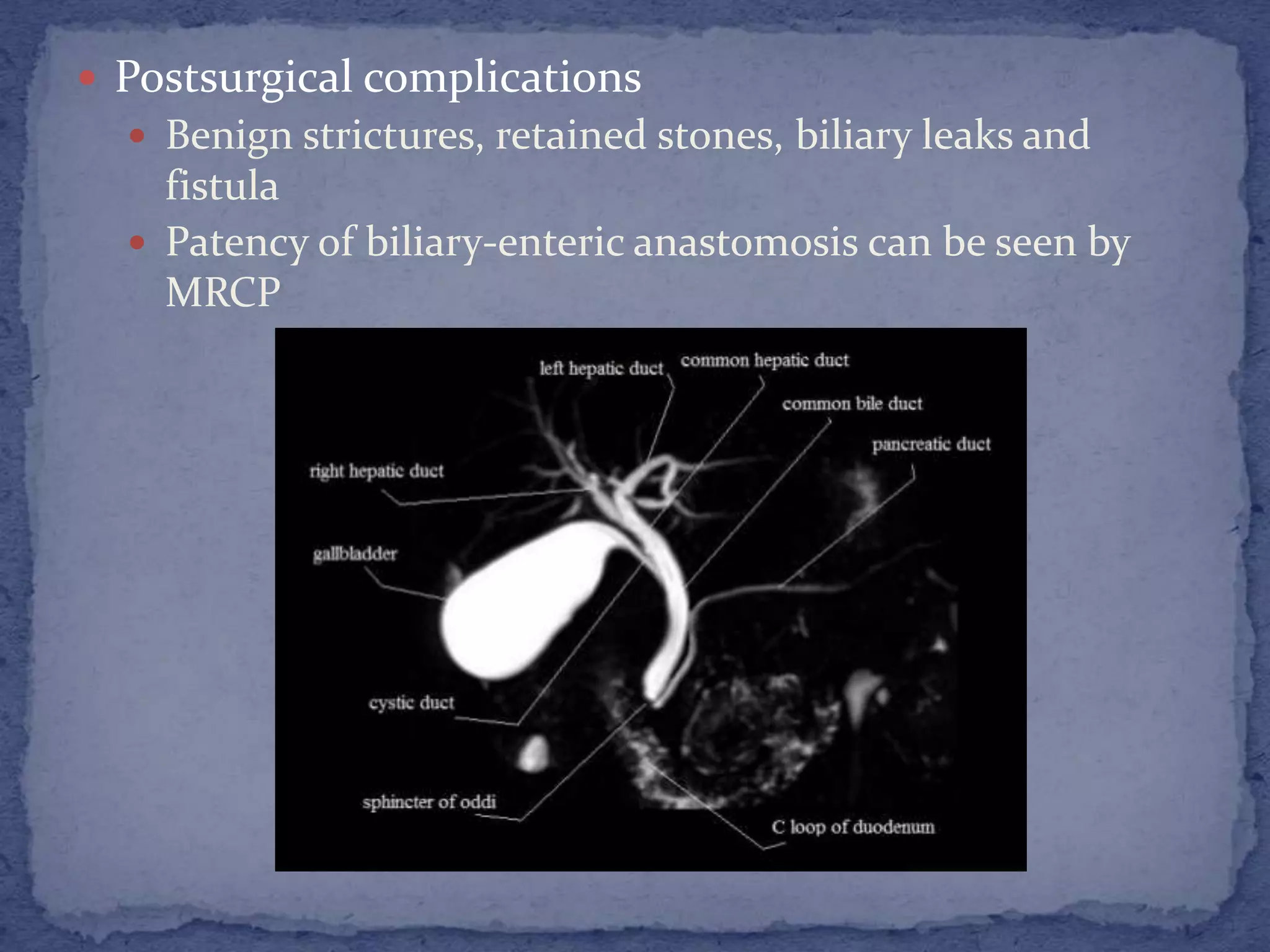

MRCP is a non-invasive imaging technique that uses heavily T2-weighted sequences to visualize the biliary and pancreatic ducts without the need for contrast injection or radiation. Various sequences such as 3D FSE, single-shot FSE, and balanced SSFP can be used to produce images with high resolution and without motion artifacts. MRCP is useful for diagnosing and evaluating cystic duct abnormalities, gallstones, pancreatic and biliary strictures, leaks, tumors and other conditions affecting the biliary tree or pancreas.








































![MAGNETIC_RESONANCE_CHOLANGIOPANCREATOGRAPHY_(MRCP)[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/magneticresonancecholangiopancreatographymrcp1-251005181226-e267a8ec-thumbnail.jpg?width=640&height=640&fit=bounds)






































