INTRODUCTION
It is adiagnostic and interventional procedure technique
using both endoscopy and fluoroscopy for examination
and intervention of the biliary tree and pancreatic ducts.
It is typically performed by doctors with endoscopic
qualifications (e.g. general surgeons, gastroenterologists)
rather than radiologists.
The contrast media is injected into the common bile duct
and the pancreatic duct through a catheter that is passed
down an endoscope.
3.
INDICATIONS
Post cholecystectomysyndrome.
Biliary drainage.
Bile duct stones removal (e.g. choledocholithiasis).
Biliary stenting for strictures and leakage.
Biliary or pancreatic ductal system tissue sampling.
Triple tissue sampling (TTS) is a common practice.
Manometry for sphincter of Oddi.
Balloon dilation of the duodenal papilla or ductal
strictures.
Sphincterotomy (e.g. sphincter of Oddi dysfunction or
stenosis)
4.
CONTD……
Management ofbile duct stones.
Management of benign and malignant biliary
strictures.
Evaluation of ampullary lesions.
Diagnostic cholangiography in patients
unsuitable/intolerant of MRCP and in whom
endoscopic ultrasound is inconclusive or unavailable.
Treatment and evaluation of chronic pancreatitis.
Investigation of diffuse biliary disease, e.g.
sclerosing cholangitis.
5.
CONTRAINDICATIONS
COMMON
• Oesophageal obstruction;pyloric stenosis/gastric or duodenal
obstruction
• Previous gastric surgery that complicates access to the duodenum
• Severe cardiac/respiratory disease.
RELATIVE
• Altered anatomy in post-surgical states (e.g. Billroth II
gastrojejunostomy, Roux-en-Y jejunostomy)
• Structural abnormalities of oesophagus, stomach or
• duodenum
• Coagulopathy
ABSOLUTE
• Unstable patient
6.
PATIENT PREPARATION
– Patientis advised not eat, drink or smoke for at least six
hours before the procedure.
– Fluids like water can be taken.
– Explain the procedure to the patient.
– Take patients consent for the same or if the patient is not
able to understand the an attendant or a guardian is supposed
to give the consent.
– Remove all the metallic objects present in the vicinity of
the examination.
– Ask the patient to change into a hospital gown
7.
EQUIPMENT
Side-viewing ENDOSCOPE
FLUOROSCOPIC UNIT with spot
image facilities.
Polythene catheter.
Guidewire in some cases.
Contrast.
Sedatives(50-100 mg xylocaine
spray).
Buscopan.
8.
CONTRAST
Pancreas
❑ LOCM 240/300mgI/mL
Bile Ducts
❑ LOCM 150 mgI/mL; dilute contrast medium so
that calculi will not be obscured.
9.
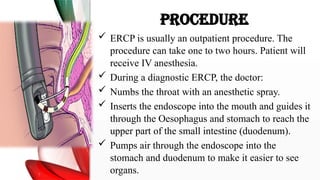
PROCEDURE
ERCP isusually an outpatient procedure. The
procedure can take one to two hours. Patient will
receive IV anesthesia.
During a diagnostic ERCP, the doctor:
Numbs the throat with an anesthetic spray.
Inserts the endoscope into the mouth and guides it
through the Oesophagus and stomach to reach the
upper part of the small intestine (duodenum).
Pumps air through the endoscope into the
stomach and duodenum to make it easier to see
organs.
10.
CONTD……
– Slides acatheter, into the endoscope until it reaches
the bile and pancreatic ducts.
– Injects the CM through the catheter.
– Takes gastrointestinal X-rays (fluoroscopy) as the CM
travels through the ducts.
– Checks for signs of blockage or problems.
– For treatment, the doctor may insert tiny instruments
through the endoscope to:
• Break up and remove stones.
• Place stents to open blocked or narrowed ducts.
• Remove tumors or tissue samples to biopsy.
13.
IMAGING
Preliminary Image ProneAP and left anterior oblique (LAO) of
the upper abdomen, to check for opaque gallstones and pancreatic
calcification/ calculi
– Pancreas (using fine focal spot)
• Prone, both posterior obliques.
– Bile ducts
1. Early filling images to show calculi: (a) Prone—straight and
posterior obliques (b) Supine—straight, both obliques; Trendelenburg
to fill intrahepatic ducts; semi-erect to fill lower
end of common bile duct and gallbladder.
2. Images following removal of the endoscope, which may
obscure the duct.
3. Delayed images to assess the gallbladder and emptying of the
common bile duct
15.
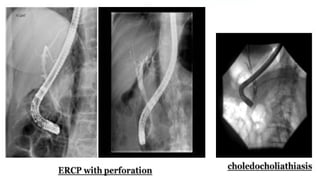
COMPLICATIONS
Pancreatitis (~5%)
Haemorrhage.
Perforation leading to pneumoperitoneum and/or
pneumoretroperitoneum
Infection (e.g. cholangitis).
Migration of a biliary or pancreatic duct stent
Complications secondary to endoscopy e.g.
oesophageal and gastric injury
16.
AFTERCARE
o Nil orallyuntil conscious and sensation has returned
to the pharynx (usually <1 hour)
o Pulse, temperature and blood pressure half-hourly
for 6 h
o Maintain antibiotics if there is biliary or pancreatic
obstruction
o Serum/urinary amylase if pancreatitis is suspected

























![definitio products ercp-180612090109[1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ercp-18061209010911-250602134305-959596a5-thumbnail.jpg?width=640&height=640&fit=bounds)
![define products of ercp-180612090109[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ercp-1806120901091-250602131957-578ccac8-thumbnail.jpg?width=640&height=640&fit=bounds)
![ercp-180612ewdhehwjbfew090109[1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ercp-18061209010911-250602134756-35275575-thumbnail.jpg?width=640&height=640&fit=bounds)




























