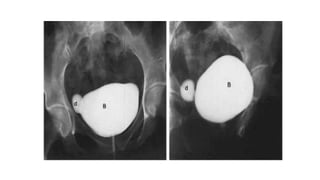
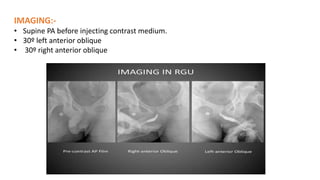
Micturating Cystourethrography (MCU) and Retrograde Urethrography (RGU) are imaging techniques used to evaluate the lower urinary tract. MCU involves filling the bladder with contrast and imaging the bladder and urethra during voiding. RGU involves retrograde injection of contrast through the urethra. Both techniques can detect abnormalities of the bladder, urethra, and identify vesicoureteral reflux. Precise technique and imaging in multiple planes are required to fully evaluate the lower urinary tract. Potential complications include infection, contrast reaction, and trauma.















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

